NCLEX-RN Practice Test Questions


You've learned about the NCLEX-RN exam, studied the sections, and are ready to put your knowledge to the test. Take our practice NCLEX exam below to get ready for the real deal.
Jump to Section
Click on the section names below to jump to a particular section of the RegisteredNursing.org NCLEX-RN Practice Exam.
- The Safe and Effective Care Environment: The Management of Care
- The Safe and Effective Care Environment: Safety and Infection Control
- Health Promotion and Maintenance
- Psychosocial Integrity
- Physiological Integrity: Basic Care and Comfort
- Physiological Integrity: Pharmacological and Parenteral Therapies
- Physiological Integrity: Reduction of Risk Potential
- Physiological Integrity: Physiological Adaptation
The NCLEX-RN Test Plan is organized into four major Client Needs categories. Two of the four categories are divided into subcategories as shown below:
- Safe and Effective Care Environment
- Management of Care – 17% to 23%
- Safety and Infection Control – 9% to 15%
- Health Promotion and Maintenance – 6% to 12%
- Psychosocial Integrity – 6% to 12%
- Physiological Integrity
- Basic Care and Comfort – 6% to 12%
- Pharmacological and Parenteral Therapies – 12% to 18%
- Reduction of Risk Potential – 9% to 15%
- Physiological Adaptation – 11% to 17%
For more practice test questions from professional sources try these.

The Safe & Effective Care Environment: The Management of Care Practice Questions
- You should respond to the couple by stating that only unanticipated treatments and procedures that are not included in the advance directive can be made by the legally appointed durable power of attorney for healthcare decisions.
- You should be aware of the fact that the wife of the client has a knowledge deficit relating to advance directives and durable powers of attorney for healthcare decisions and plan an educational activity to meet this learning need.
- You should be aware of the fact that the client has a knowledge deficit relating to advance directives and durable powers of attorney for healthcare decisions and plan an educational activity to meet this learning need.
- You should reinforce the wife’s belief that legally married spouses automatically serve for the other spouse’s durable power of attorney for health care decisions and that others than the spouse cannot be legally appointed while people are married
Correct Response: A
You should respond to the couple by stating that only unanticipated treatments and procedures that are not included in the advance directive can be made by the legally appointed durable power of attorney for healthcare decisions.
Both the client and the client’s spouse have knowledge deficits relating to advance directives. Legally married spouses do not automatically serve for the other spouse’s durable power of attorney for health care decisions; others than the spouse can be legally appointed while people are married.
- Privacy and to have their medical information confidential unless the client formally approves the sharing of this information with others such as family members.
- Make healthcare decisions and to have these decisions protected and communicated to others when they are no longer competent to do so.
- Be fully informed about all treatments in term of their benefits, risks and alternatives to them so the client can make a knowledgeable and informed decision about whether or not to agree to having it
- Make decisions about who their health care provider is without any coercion or undue influence of others including healthcare providers.
Correct Response: B,D
The Patient Self Determination Act, which was passed by the US Congress in 1990, gives Americans the right to make healthcare decisions and to have these decisions protected and communicated to others when they are no longer competent to do so. These decisions can also include rejections for future care and treatment and these decisions are reflect in advance directives. This Act also supports the rights of the client to be free of any coercion or any undue influence of others including healthcare providers.
The Health Insurance Portability and Accountability Act (HIPAA) supports and upholds the clients’ rights to confidentially and the privacy of their medical related information regardless of its form. It covers hard copy and electronic medical records unless the client has formally approved the sharing of this information with others such as family members.
The elements of informed consent which includes information about possible treatments and procedures in terms of their benefits, risks and alternatives to them so the client can make a knowledgeable and informed decision about whether or not to agree to having it may be part of these advanced directives, but the law that protects these advance directives is the Patient Self Determination Act.
- Call the doctor and advise them that the client’s physical status has significantly changed and that they have just had a cardiopulmonary arrest.
- Begin cardiopulmonary resuscitation other emergency life saving measures.
- Notify the family of the client’s condition and ask them what they should be done for the client.
- Insure that the client is without any distressing signs and symptoms at the end of life.
Correct Response: B
You must immediately begin cardiopulmonary resuscitation and all life saving measures as requested.by the client in their advance directive despite the nurse’s own beliefs and professional opinions. Nurses must uphold the client’s right to accept, choose and reject any and all of treatments, as stated in the client’s advance directive.
You would not call the doctor first; your priority is the sustaining of the client’s life; you would also not immediately notify the family for the same reason and, when you do communicate with the family at a later time, you would not ask them what should or should not be done for the client when they wishes are already contained in the client’s advance directive.
Finally, you would also insure that the client is without pain and all other distressing signs and symptoms at the end of life, but the priority and the first thing that you would do is immediately begin cardiopulmonary resuscitation and all life saving measures as requested by the client in their advance directive, according to the ABCs and Maslow’s Hierarchy of Needs.
- Case manager
- Collaborator
- Coordinator of care
- Advocacy
Correct Response: D
The priority role of the nurse is advocacy. The nurse must serve as the advocate for both the fetus and the mother at risk as the result of this ethical dilemma where neither option is desirable. As an advocate, the nurse would seek out resources and people, such as the facility’s ethicist or the ethics committee, to resolve this ethical dilemma.
- Client advocate
- Collaborator
- Politician
- Entrepreneur
Correct Response: A
A nurse who organizes and establishes a political action committee (PAC) in their local community to address issues relating to the accessibility and affordability of healthcare resources in the community is serving as the client advocate. As you should know, the definition of “client” includes not only individual clients, and families as a unit, but also populations such as the members of the local community.
Although the nurse, as the organizer of this political action committee (PAC), will have to collaborate with members of the community to promote the accessibility and affordability of healthcare resources in the community, this is a secondary role rather than the primary role.
Additionally, although the nurse is serving in a political advocacy effort, the nurse is not necessarily a politician and there is no evidence that this nurse is an entrepreneur.
- The right task, the right circumstances, the right person, the right competency, and the right supervision or feedback
- The right task, the right circumstances, the right person, the right direction or communication, and the right supervision or feedback
- The right competency, the right education and training, the right scope of practice, the right environment and the right client condition
- The right competency, the right person, the right scope of practice, the right environment and the right client condition
Correct Response: B
The Five Rights of Delegation include the right task, the right circumstances, the right person, the right direction or communication, and the right supervision or feedback.
The right competency is not one of these basic Five Rights, but instead, competency is considered and validated as part of the combination of matching the right task and the right person; the right education and training are functions of the right task and the right person who is able to competently perform the task; the right scope of practice, the right environment and the right client condition are functions of the legal match of the person and the task; and the setting of care which is not a Right of Delegation and the matching of the right person, task and circumstances.
- The American Nurses Association’s Scopes of Practice
- The American Nurses Association’s Standards of Care
- State statutes
- Federal law
Correct Response: C
The registered nurse, prior to the delegation of tasks to other members of the nursing care team, evaluates the ability of staff members to perform assigned tasks for the position as based on state statutes that differentiate among the different types of nurses and unlicensed assistive personnel that are legally able to perform different tasks.
Although the American Nurses Association’s Standards of Care guide nursing practice, these standards are professional rather than legal standards and the American Nurses Association does not have American Nurses Association’s Scopes of Practice, only the states’ laws or statutes do.
Lastly, scopes of practice are within the legal domain of the states and not the federal government.
- Observe the staff member during an entire shift of duty to determine whether or not the nurse has accurately and appropriately established priorities.
- Observe the staff member during an entire shift of duty to determine whether or not the nurse has accurately and appropriately completed priority tasks.
- Ask the staff member how they feel like they have been able to employ their time management skills for the last six months.
- Collect outcome data over time and then aggregate and analyze this data to determine whether or not the staff member has completed reasonable assignments in the allotted time before the end of their shift of duty.
Correct Response: D
The best way to objectively evaluate the effectiveness of an individual staff member’s time management skills in a longitudinal manner is to collect outcome data over time, and then aggregate and analyze this data to determine whether or not the staff member has completed reasonable assignments in the allotted time before the end of their shift of duty. Another way to perform this longitudinal evaluation is to look at the staff member’s use of over time, like the last six months, when the unit was adequately staffed.
Observing the staff member during an entire shift of duty to determine whether or not the nurse has accurately and appropriately established priorities is a way to evaluate the short term abilities for establishing priorities and not assignment completion and observing the staff member during an entire shift of duty to determine whether or not the nurse has accurately and appropriately completed priority tasks is a way to evaluate the short term abilities for completing established priorities and not a complete assignment which also includes tasks that are not of the highest priority.
Lastly, asking the staff member how they feel like they have been able to employ their time management skills for the last six months is the use of subjective rather than objective evaluation.
- An unlicensed staff member who has been “certified” by the employing agency to monitor telemetry: Monitoring cardiac telemetry
- An unlicensed assistive staff member like a nursing assistant who has been “certified” by the employing agency to insert a urinary catheter: Inserting a urinary catheter
- A licensed practical nurse: The circulating nurse in the perioperative area
- A licensed practical nurse: The first assistant in the perioperative area
Correct Response: A
An unlicensed staff member who has been “certified” by the employing agency to monitor telemetry can monitor cardiac telemetry; they cannot, however, interpret these cardiac rhythms and initiate interventions when interventions are indicated. Only the nurse can perform these roles.
Unlicensed assistive staff member like a nursing assistant cannot under any circumstances be certified” by the employing agency to insert a urinary catheter or insert a urinary catheter because this is a sterile procedure and, legally, no sterile procedures can be done by an unlicensed assistive staff member like a nursing assistant.
Lastly, the role of the circulating nurse is within the exclusive scope of practice for the registered nurse and the role of the first assistant is assumed only by a registered nurse with the advanced training and education necessary to perform competently in this capacity. Neither of these roles can be delegated to a licensed practical nurse or an unlicensed assistive staff member like a nursing assistant or a surgical technician.
- Only the VA health care services because he is not 65 years of age
- Medicare because he has been deemed permanently disabled for 2 years
- Medicaid because he is permanently disabled and not able to work
- Choices B and C
Correct Response: B
This client is legally eligible for Medicare because he has been deemed permanently disabled for more than 2 years in addition to the VA health care services. People over the age of 65 and those who are permanently disabled for at least two years, according to the Social Security Administration, are eligible for Medicare.
Based on the information in this scenario, the client is not eligible for Medicaid because has a “substantial” VA disability check on a monthly basis and is not indigent and with a low income.
- The case manager’s role in terms of organization wide performance improvement activities
- The case manager’s role in terms complete, timely and accurate documentation
- The case manager’s role in terms of the clients’ being at the appropriate level of care
- The case manager’s role in terms of contesting denied reimbursements
Correct Response: C
Registered nurse case managers have a primary case management responsibility associated with reimbursement because they are responsible for insuring that the client is being cared for at the appropriate level of care along the continuum of care that is consistent with medical necessity and the client’s current needs. A failure to insure the appropriate level of care jeopardizes reimbursement. For example, care in an acute care facility will not be reimbursed when the client’s current needs can be met in a subacute or long term care setting.
Nurse case managers do not have organization wide performance improvement activities, the supervision of complete, timely and accurate documentation or challenging denied reimbursements in their role. These roles and responsibilities are typically assumed by quality assurance/performance improvement, supervisory staff and medical billers, respectively.
- The ProACT Model: Registered nurses perform the role of the primary nurse in addition to the related coding and billing functions
- The Collaborative Practice Model: The registered nurse performs the role of the primary nurse in addition to the role of the clinical case manager with administrative, supervisory and fiscal responsibilities
- The Case Manager Model: The management and coordination of care for clients throughout a facility who share the same DRG or medical diagnosis
- The Triad Model of Case Management: The joint collaboration of the social worker, the nursing case manager, and the utilization review team
Correct Response: D
The Triad Model of case management entails the joint collaboration of the social worker, the nursing case manager, and the utilization review team.
The Professionally Advanced Care Team, referred to as the ProACT Model, which was developed at the Robert Wood Johnson University Hospital, entails registered nurses serving in the role of both the primary nurse the clinical case manager with no billing and coding responsibilities; these highly specialized and technical billing and coding responsibilities are done by the business office, medical billers and medical coders.
The Case Manager Model entails the registered nurses’ role in terms of case management for a particular nursing care unit for a group of clients with the same medical diagnosis or DRG. In contrast to this Case Manager Model of Beth Israel Hospital, the Collaborative Practice Model of case management entails the role of some registered nurses in a particular healthcare facility to manage, coordinate, guide and direct the complex care of a population of clients throughout the entire healthcare facility who share a particular diagnosis or Diagnostic Related Group.
- The Case Manager Model
- The ProACT Model
- The Collaborative Practice Model
- The Triad Model of Case Management
Correct Response: A
The Case Manager Model and the Collaborative Practice Model of case management are the only models of case management that employ the mandated and intrinsic use of critical pathways which are multidisciplinary plans of care that are based on the client’s current condition, and that reflect interventions and expected outcomes within a pre-established time line.
The ProACT Model, the Collaborative Practice Model and the Triad Model of Case Management do not necessarily employ critical pathways; these models can use any system of medical records and documentation.
- An opt out consent
- An implicit consent
- An explicit consent
- No consent at all is given
Correct Response: B
The type of legal consent that is indirectly given by the client by the very nature of their voluntary acute care hospitalization is an implicit consent indirectly given by the client by the very nature of their voluntary acute care hospitalization is an implicit consent.
An explicit consent, on the other hand, is the direct and formal consent of the client; and an opt out consent is given when a patient does NOT refuse a treatment; this lack of objections by the patient indicates that the person has consented to the treatment or procedure with an opt out consent.
- Take the photographs because these photographs are part of the holiday tradition at this facility
- Take the photographs because all of the residents are properly attired and in a dignified condition
- Refuse to take the photographs unless you have the consent of all to do so
- Refuse to take the photographs because this is not part of the nurse’s role
Correct Response: C
You should refuse to take the photographs unless you have the consent of all to do so because to do otherwise is a violation of the residents’ rights to privacy and confidentiality as provided in the Health Insurance Portability and Accountability Act (HIPAA). This, rather than the false belief that this is not part of the nurse’s role, is the reason that you would not automatically take these photographs.
Regardless of whether or not these photographs are part of the holiday tradition at this facility and whether or not the residents are properly attired and in a dignified condition, no photographs can be legally taken without the residents’ permission and consent.
- The Patient Self Determination Act: The client’s right to choose the level of care
- The Patient Self Determination Act: The clients’ right to healthcare insurance coverage for mental health disorders
- The Mental Health Parity Act: The privacy and security of technological psychiatric information
- The Health Insurance Portability and Accountability Act (HIPAA): The privacy and security of technological medical information
Correct Response: D
The Health Insurance Portability and Accountability Act (HIPAA) protects the client’s legal rights to the privacy, security and confidentiality of all medical information including data and information that is technologically stored and secured.
The Patient Self Determination Act uphold the client’s right to choose and reject care and not the level of care that is driven and decided upon as based on medical necessity and health insurance reimbursement; this Act also does not give client’s the right to any health insurance including healthcare insurance coverage for mental health disorders.
Lastly, the Mental Health Parity and Addiction Equality Act, passed in 2008, mandates insurance coverage for mental health and psychiatric health services in a manner similar to medical and surgical insurance coverage; it does not protect the privacy and security of technological psychiatric information, HIPAA does.
- The physical therapist
- The occupational therapist
- The podiatrist
- The nurse practitioner
Correct Response: A
The member of the multidisciplinary team that you would most likely collaborate with when the client is at risk for falls due to an impaired gait is a physical therapist. Physical therapists are licensed healthcare professionals who assess, plan, implement and evaluate interventions including those related to the patient’s functional abilities in terms of their gait, strength, mobility, balance, coordination, and joint range of motion. They also provide patients with assistive aids like walkers and canes and exercise regimens.
Occupational therapists assess, plan, implement and evaluate interventions including those that facilitate the patient’s ability to achieve their highest possible level of independence in terms of their activities of daily living such as bathing, grooming, eating and dressing.
Podiatrists care for disorders and diseases of the foot; and nurse practitioners, depending on their area of specialty, may also collaborate with nurses when a client is affected with a disorder in terms of gait, strength, mobility, balance, coordination, and joint range of motion, however the member of the multidisciplinary team that you would most likely collaborate with when the client is at risk for falls due to an impaired gait is a physical therapist.
- The physical therapist
- The occupational therapist
- The dietician
- The podiatrist
Correct Response: B
The member of the multidisciplinary team that you would most likely collaborate with when the client can benefit from the use of adaptive devices for eating is the occupational therapist. Occupational therapists assess, plan, implement and evaluate interventions including those that facilitate the patient’s ability to achieve their highest possible level of independence in terms of their activities of daily living such as bathing, grooming, eating and dressing. Many of these interventions include adaptive devices such as special eating utensils and grooming aids.
Physical therapists are licensed healthcare professionals who assess, plan, implement and evaluate interventions including those related to the patient’s functional abilities in terms of their gait, strength, mobility, balance, coordination, and joint range of motion. They also provide patients with assistive aids like walkers and canes and exercise regimens.
Dieticians assess, plan, implement and evaluate interventions including those relating to dietary needs of those patients who need regular or therapeutic diets. They also provide dietary education and work with other members of the healthcare need when a client has dietary needs secondary to physical disorders such as dysphagia; and podiatrists care for disorders and diseases of the foot.
- To fulfill the nurse’s role in terms of collaboration
- To plan and provide for optimal client outcomes
- To solve complex multidisciplinary patient care problems
- To provide educational experiences for experienced nurses
Correct Response: C
The primary goal of multidisciplinary case conferences is to plan care that facilitates optimal client outcomes. Other benefits of multidisciplinary case conferences include the fulfillment of the nurse’s role in terms of collaboration and collegiality, to solve complex multidisciplinary patient care problems so that optimal client outcomes can be achieved and also to provide educational experiences for nurses; these things are secondary rather than primary goals.
- A Pedorthist
- A pediatric nurse practitioner
- A trauma certified clinical nurse specialist
- A prosthetist
Correct Response: D
The member of the multidisciplinary team would you most likely collaborate with when your pediatric client has had a traumatic amputation secondary to a terrorism blast explosion a month ago or more ago is a prosthetist. Prosthetists, in collaboration with other members of the healthcare team, assess patients and then design, fit and supply the patient with an artificial body part such as a leg or arm prosthesis. They also follow-up with patients who have gotten a prosthesis to check and adjust it in terms of proper fit, patient comfort and functioning.
Pedorthists modify and provide corrective footwear and employ supportive devices to address conditions which affect the feet and lower limbs. Lastly, you may collaborate with a trauma certified clinical nurse specialist and a pediatric nurse practitioner but this consultation and collaboration should begin immediately upon arrival to the emergency department, and not a month after the injury.
- Conceptualization conflicts
- Avoidance - Avoidance conflicts
- Approach - Approach conflicts
- Resolvable conflicts
- Unresolvable conflicts
- Double Approach - Avoidance conflicts
- Approach-Avoidance conflicts
Correct Response: B, C, F, G
According to Lewin, the types of conflict are Avoidance-Avoidance conflicts, Approach- Approach conflicts, Double Approach - Avoidance conflicts and Approach-Avoidance conflicts.
- Frustration: The phase of conflict that is characterized with personal agendas and obstruction
- Conceptualization: The phase of conflict that occurs when contending parties have developed a clear and objective understanding of the nature of the conflict and factors that have led to it
- Taking action: The phase of conflict that is characterized with individual responses to and feelings about the conflict
- Resolution: The type of conflict that can be resolved
- Avoidance-Avoidance: A stage of conflict that occurs when there are NO alternatives that are acceptable to the contending parties
- Approach- Approach Conflicts: The type of conflict that occurs when the people involved in the conflict want more than one alternatives or actions that could resolve the conflict.
- Approach-Avoidance Conflicts: The type of conflict that occurs when the people involved in the conflict believe that all of the alternatives are NEITHER completely satisfactory nor completely dissatisfactory.
Correct Response: C, F, G
Taking action is the phase of conflict that is characterized with individual responses to and feelings about the conflict; Approach- Approach conflicts are a type of conflict that occurs when the people involved in the conflict want more than one alternatives or actions that could resolve the conflict; and Approach-Avoidance conflicts are a type of conflict that occurs when the people involved in the conflict believe that all of the alternatives are NEITHER completely satisfactory or completely dissatisfactory.
Frustration is the phase of conflict that occurs when those involved in the conflict believe that their goals and needs are being blocked and not met, and not necessarily characterized with personal agendas and obstruction; conceptualization is the phase of conflict that occurs when those involved in the conflict begin to understand what the conflict is all about and why it has occurred. This understanding often varies from person to person and this personal understanding may or may not be accurate, clear or objective, and not a clear and objective understanding of the nature of the conflict and factors that have led to it; resolution is a phase of conflict resolution, not a type of conflict, that is characterized when the contending parties are able to come to some agreement using mediation, negotiation or another method; an Avoidance-Avoidance conflict is a type of conflict and not a phase of conflict, that occurs when there are NO alternatives that are acceptable to any the contending parties; Approach- Approach conflicts occur when the people involved in the conflict want more than one alternative or action that could resolve the conflict; and lastly, Double Approach - Avoidance is a type of conflict and not a stage of conflict that occurs when the people involved in the conflict are forced to choose among alternatives and actions, all of which have BOTH positive and negative aspects to them.
- Passivity
- Compromise
- Competition
- Accommodating Others
Correct Response: B
Conflicts can be effectively resolved using a number of different strategies and techniques such as compromise, negotiation, and mediation.
Avoidance of the conflict, withdrawing in addition to other passivity, competition, and accommodating others are not effective and healthy conflict resolution techniques.
- Conceptualization
- Frustration
- Resolution
- Taking action
Correct Response: B, A, D, C
The stages of conflict and conflict resolution in the correct sequential order are frustration, conceptualization, and taking action.
- The Patient Self Determination Act
- The Mental Health Parity Act
- The Health Insurance Portability and Accountability Act
- The Americans with Disabilities Act of 1990
Correct Response: C
The federal law is most closely associated with the highly restrictive “need to know” is the Health Insurance Portability and Accountability Act. This law restricts access to medical information to only those persons who have the need to know this information in order to provide direct and/or indirect care to the client.
The Patient Self Determination Act, which was passed by the US Congress in 1990, gives Americans the right to make healthcare decisions and to have these decisions protected and communicated to others when they are no longer competent to do so. These decisions can also include rejections for future care and treatment and these decisions are reflect in advance directives. This Act also supports the rights of the client to be free of any coercion or any undue influence of others including healthcare providers.
The Mental Health Parity Act passed in 2008, mandates insurance coverage for mental health and psychiatric health services in a manner similar to medical and surgical insurance coverage.
And, lastly the Americans with Disabilities Act of 1990 and the Rehabilitation Act of 1973 forbid and prohibit any discrimination against people with disabilities.
- The facility’s Performance Improvement Director who is not a healthcare person and who has no direct contact with clients
- A nursing student who is caring for a client under the supervision of the nursing instructor
- The facility’s Safety Officer who is not a healthcare person and who has no direct contact with clients
- A department supervisor with no direct or indirect care duties
Correct Response: D
A department supervisor with no direct or indirect care duties does not have the “right to know” medical information; all of the others have the “right to know” medical information because they provide direct or indirect care to clients.
For example, both the facility’s Performance Improvement Director who is not a healthcare person and who has no direct contact with clients and the facility’s Safety Officer who is not a healthcare person and who has no direct contact with clients provide indirect care to clients. For example, they collect and analyze client data in order to fulfill their role and responsibilities in terms of process improvements and the prevention of incidents and accidents, respectively.
Nursing and other healthcare students also have the “need to know” medical information so that they can provide direct client care to their assigned client(s).
- “A computer in the hallway was left unattended and a client’s medical record was visible to me.”
- “I just saw a nursing student looking at the medical record for a client that they are NOT caring for during this clinical experience.”
- “As I was walking past the nursing station, I saw a dietician reading the progress notes written by members of the laboratory department in addition to other dieticians’ progress notes.”
- “I refused the nursing supervisor’s request to share my electronic password for the new nurse on the unit.”
Correct Response: C
A staff members comment, “As I was walking past the nursing station, I saw a dietician reading the progress notes written by members of the laboratory department in addition to other dieticians’ progress notes” “indicates the need for the Nurse Manager to provide an educational activity relating to confidentiality and information security because dieticians often have the “need to know” about laboratory data so that they can, for example, assess the client’s nutritional status in terms of their creatinine levels.
The report that the nursing student was “looking at the medical record for a client that they are NOT caring for during this clinical experience” indicates that the reporting staff member is correctly applying the principles for maintaining confidentiality and privacy of information; the report that a “computer in the hallway was left unattended and a client’s medical record was visible to me” indicates that the reporting staff member is correctly applying the principles for maintaining confidentiality and privacy of information; and lastly, “I refused the nursing supervisor’s request to share my electronic password for the new nurse on the unit” also indicates that the staff member is knowledgeable about privacy and confidentiality.
- Case management
- Continuity of care
- Medical necessity
- Critical pathway
Correct Response: B
The continuity of care is defined as the sound, timely, smooth, unfragmented and seamless transition of a client from one area within the same healthcare facility, from one level of care to a higher and more intense level of care or to a less intense level of care based on the client’s status and level of acuity, from one healthcare facility to another healthcare facility and also any discharges to the home in the client’s community.
Case management and critical pathways may be used to facilitate the continuity of care, but they are not the sound, timely, smooth, unfragmented and seamless transition of the client from one level of acuity to another. Lastly, medical necessity is necessary for reimbursement and it is one of the considerations for moving the client from one level of acuity to another but medical necessity is not the continuity of care.
- The Four P's
- UBAR
- ISBAR
- MAUMAR
Correct Response: C
The standardized “hand off” change of shift reporting system that you may want to consider for implementation on your nursing care unit is ISBAR. Other standardized change of shift “hand off” reports, as recommended by the Joint Commission on the Accreditation of Healthcare Organization, include:
- SBAR, not IBAR
- BATON
- The Five Ps not the Four Ps and
- IPASS
Lastly, MAUUAR is a method of priority setting and not a standardized “hand off” change of shift reporting system.
- SBAR: Symptoms, background, assessment and recommendations
- ISBAR: Interventions, symptoms, background, assessment and recommendations
- The Five Ps: The patient, plan, purpose, problems and precautions
- BATON: Background, assessment, timing, ownership and next plans
Correct Response: C
The Five Ps are the patient, plan, purpose, problems and precautions.
The elements of the other standardized reporting systems are listed below:
SBAR stands for:
- S: Situation: The patient’s diagnosis, complaint, plan of care and the patient's prioritized needs
- B: Background: The patient’s code or DNR status, vital Signs, medications and lab results
- A: Assessment: The current assessment of the situation and the patient’s status and
- R: Recommendations: All unresolved issues including things like pending diagnostic testing results and what has to be done over the next few hours
ISBAR stands for:
- I: Introduction: The introduction of the nurse, the nurse’s role in care and the area or department that you are from
- S: Situation: The patient’s diagnosis, complaint, plan of care and the patient's prioritized needs
- B: Background: The patient’s code or DNR status, vital Signs, medications and lab results
- A: Assessment: The current assessment of the situation and the patient’s status and
- R: Recommendations: All unresolved issues including things like pending diagnostic testing results and what has to be done over the next few hours
BATON stands for:
- B: Background: Past and current medical history, including medications
- A: Actions: What actions were taken and/or those actions that are currently required
- T: Timing: Priorities and level of urgency
- O: Ownership: Who is responsible for what? and
- N: Next: The future plan of care
IPASS stands for:
- Introduction: The introduction of the nurse, the nurse’s role in care and the area or department that you are from
- P: Patient: The patient’s name, age, gender, location and other demographic data
- A: Assessment: The current assessment of the situation and the patient’s status
- S: Situation: The patient’s diagnosis, complaint, plan of care and the patient's prioritized needs and
- S: Safety concerns: Physical, mental and social risks and concerns
- Atrial fibrillation
- First degree heart block
- Shortness of breath upon exertion
- An obstructed airway
- Fluid needs
- Respect and esteem by others
- 3,4,2,1,5,6
- 3,4,5,1,2,6
- 2,3,5,1,4,6
- 3,2,4,1,5,6
Correct Response:
Client needs are prioritized in a number of different ways including Maslow’s Hierarchy of Human Needs and the ABCs. In terms of priorities from # 1 to # 6 the conditions above are prioritized as follows:
- An obstructed airway
- First degree heart block
- Atrial fibrillation
- Shortness of breath upon exertion
- Fluid needs
- Respect and esteem by others
The ABCs identifies the airway, breathing and cardiovascular status of the patient as the highest of all priorities in that sequential order; and Maslow’s Hierarchy of Needs identifies the physiological or biological needs, including the ABCs, the safety/psychological/emotional needs, the need for love and belonging, the needs for self-esteem and the esteem by others and the self-actualization needs in that order of priority.
- Assessment
- Movement
- Understanding level
- Risks
Correct Response: D
One of the 2nd priority needs according to the MAAUAR method of priority setting is risks.
The ABCs / MAAUAR method of priority setting places the ABCs, again, as the highest and greatest priorities which are then followed with the 2nd and 3rd priority level needs of the MAAUAR method of priority setting.
The 2nd priority needs according to the MAAUAR method of priority setting after the ABCs include M-A-A-U-A-R which stands for:
- Mental status changes and alterations
- Acute pain
- Acute urinary elimination concerns
- Unaddressed and untreated problems that require immediate priority attention
- Abnormal laboratory and other diagnostic data that are outside of normal limits and
- Risks including those relating to a healthcare problem like safety, skin breakdown, infection and other medical conditions
The 3rd level priorities include all concerns and problems that are NOT covered under the 2nd level priority needs and the ABCs. For example, increased levels of self care abilities and skills and enhanced knowledge of a medical condition are considered 2nd level priority needs.
- Time management skills
- Communication skills
- Collaboration skills
- Supervision skills
Correct Response: A
Time management skills are most closely related to successfully meeting the established priority needs of a group of clients.
In addition to prioritizing and reprioritizing, the nurse should also have a plan of action to effectively manage their time; they should avoid unnecessary interruptions, time wasters and helping others when this helping others could potentially jeopardize their own priorities of care.
Although good communication skills, collaboration skills and supervision are necessary for the delivery of nursing care, it is time management skills that are most closely related to successfully meeting the established priority needs of a group of clients.
- Morals
- Laws
- Statutes
- Client rights
Correct Response: A
Morals are most closely aligned with ethics. Ethics is a set of beliefs and principles that guide us in terms of the right and wrong thing to do which is the most similar to ethics.
Laws and statutes defined what things are legal and what things are illegal. Lastly, client rights can serve as a factor to consider when ethical decisions are made; but they are not most closely aligned with ethics, but only, one consideration of many that can be used in ethical decision making.
- Deontology: The school of ethical of thought that requires that only the means to the goal must be ethical.
- Utilitarianism: The school of ethical of thought that requires that only the end goal must be ethical.
- Deontology: The school of ethical of thought that requires that only the end goal must be ethical.
- Utilitarianism: The school of ethical of thought that requires that only the means to the goal must be ethical.
Correct Response: B
The two major classifications of ethical principles and ethical thought are utilitarianism and deontology. Deontology is the ethical school of thought that requires that both the means and the end goal must be moral and ethical; and the utilitarian school of ethical thought states that the end goal justifies the means even when the means are not moral.
- Justice: Equally dividing time and other resources among a group of clients
- Beneficence: Doing no harm during the course of nursing care
- Veracity: Fully answering the client’s questions without any withholding of information
- Fidelity: Upholding the American Nurses Association’s Code of Ethics
Correct Response: C
Fully answering the client’s questions without any withholding of information is an example of the application of veracity into nursing practice. Veracity is being completely truthful with patients; nurses must not withhold the whole truth from clients even when it may lead to patient distress.
Justice is fairness. Nurses must be fair when they distribute care and resources equitably, which is not always equally among a group of patients. Beneficence is doing good and the right thing for the patient; it is nonmaleficence that is doing no harm.
- Planning a way to evaluate the effectiveness of the class by seeing a decrease in the amount of referrals to the facility’s Ethics Committee
- Establishing educational objectives for the class that reflect the methods and methodology that you will use to present the class content
- The need to exclude case studies from the class because this would violate client privacy and confidentiality
- Some of the most commonly occurring bioethical concerns including genetic engineering into the course content
Correct Response: D
You would consider including some of the most commonly occurring bioethical concerns including genetic engineering into the course content.
You would also plan how you could evaluate the effectiveness of the class by seeing an increase, not a decrease in the amount of referrals to the facility’s Ethics Committee, because one of the elements of this class should address ethical dilemmas and the role of the Ethics Committee in terms of resolving these.
You would additionally establish educational objectives for the class that reflect specific, measurable learner outcomes and not the methods and methodology that you will use to present the class content; and lastly, there is no need to exclude case studies from the class because “sanitized” medical records can, and should be, used to avoid any violations of client privacy and confidentiality.
- Serve as the witness to the client’s signature on an informed consent.
- Get and witness the client’s signature on an informed consent.
- Get and witness the durable power of attorney for health care decisions’ signature on an informed consent.
- None of the above
Correct Response: A
One of the roles of the registered nurse in terms of informed consent is to serve as the witness to the client’s signature on an informed consent.
Other roles and responsibilities of the registered nurse in terms of informed consent include identifying the appropriate person to provide informed consent for client, such as the client, parent or legal guardian, to provide written materials in client’s spoken language, when possible, to know and apply the components of informed consent, and to also verify that the client comprehends and consents to care and procedures.
The registered nurse does not get the client’s or durable power of attorney for health care decisions’ signature on an informed consent, this is the role and responsibility of the physician or another licensed independent practitioner.
- Justice
- Fidelity
- Self determination
- Nonmalficence
Correct Response: C
Self-determination is most closely aligned with the principles and concepts of informed consent. Self-determination supports the client’s right to choose and reject treatments and procedures after they have been informed and fully knowledgeable about the treatment or procedure.
Justice is fairness. Nurses must be fair when they distribute care and resources equitably, which is not always equally among a group of patients; fidelity is the ethical principle that requires nurses to be honest, faithful and true to their professional promises and responsibilities by providing high quality, safe care in a competent manner; and, lastly, nonmaleficence is doing no harm, as stated in the historical Hippocratic Oath.
- The purpose of the proposed treatment or procedure
- The expected outcomes of the proposed treatment or procedure
- Who will perform the treatment or procedure
- When the procedure or treatment will be done
Correct Response: D
The minimal essential components of the education that occurs prior to getting an informed consent include the purpose of the proposed treatment or procedure, the expected outcomes of the proposed treatment or procedure, and who will perform the treatment or procedure. It is not necessary to include when the treatment or procedure will be done at this time.
Other essential elements include:
- The benefits of the proposed treatment or procedure
- The possible risks associated with the proposed treatment or procedure
- The alternatives to the particular treatment or procedure
- The benefits and risks associated with alternatives to the proposed treatment or procedure
- The client’s right to refuse a proposed treatment or procedure
- The Security Rule
- The American Nurses Association’s Code of Ethics
- The American Hospital’s Patients’ Bill of Rights
- The Autonomy Rule
Correct Response: A
Prohibitions against sharing passwords are legally based on the Security Rule of HIPAA mandates administrative, physical, and technical safeguards to insure the confidentiality, integrity, and availability of electronic protected health information. This rule relates to electronic information security as well as other forms of information.
The American Nurses Association’s Code of Ethics and the American Hospital’s Patients’ Bill of Rights both address client confidentiality and their rights to privacy, however, these statements are not legal, but instead ethical and regulatory statements; and lastly, there is no autonomy law or rule.
- Social networks and cell phone cameras pose low risk in terms of information technology security and confidentiality.
- The security of technological data and information in healthcare environments is most often violated by those who work there.
- The security of technological data and information in healthcare environments is most often violated by computer hackers.
- Computer data deletion destroys all evidence of the data.
Correct Response: B
The security of technological data and information in healthcare environments is most often violated by those who work there. The vast majority of these violations occur as the result of inadvertent breaches with carelessness and the lack of thought on the part of employees. Technology is a double edged sword.
Technological advances such as cell phone cameras, social networks like Facebook, telephone answering machines and fax machines pose great risk in terms of the confidentiality and the security of medical information. Computer data deletion does not always destroy all evidence of the data; data remains.
- Assault: Touching a person without their consent
- Battery: Threatening to touch a person without their consent
- Slander: False oral defamatory statements.
- Slander: False written defamatory statements.
Correct Response: C
Slander is false oral defamatory statements; and libel is written defamation of character using false statements.
Assault, an intentional tort, is threatening to touch a person without their consent; and battery, another intentional tort, is touching a person without their consent.
- Ensured the client’s safety which is a high patient care priority
- Violated Respondeat Superior
- Violated the client’s right to dignity
- Committed a crime
Correct Response: D
When you loosely apply a bed sheet around your client’s waist to prevent a fall from the chair, you have falsely imprisoned the client with this make shift restraint. False imprisonment is restraining, detaining and/or restricting a person’s freedom of movement. Using a restraint without an order is considered false imprisonment even when it is done to protect the client’s safety.
Respondeat Superior is the legal doctrine or principle that states that employers are legally responsible for the acts and behaviors of its employees. Respondeat Superior does not, however, relieve the nurse of legal responsibility and accountability for their actions. They remain liable.
There is no evidence in this question that you have violated the client’s right to dignity.
- Respondeat Superior does not mean that a nurse cannot be held liable.
- Respondeat Superior does not mean that a nurse cannot be held libel.
- Respondeat Superior is an ethical principle.
- Respondeat Superior is a law.
Correct Response: A
Respondeat Superior does not mean that a nurse cannot be held liable and not libel which is a written defamation of character using false statements. Liability is legal vulnerability.
Respondeat Superior is the legal doctrine or principle and not a law or ethical principle.
- Causation, foreseeability, damages to the patient, a duty that was owed to the client and this duty was breached, and direct rather than indirect harm to the client.
- Causation, foreseeability, damages to the patient, a duty that was owed to the client and this duty was breached, and direct and/or indirect harm to the client.
- Causation, correlation, damages to the patient, a duty that was owed to the client and this duty was breached, and direct and/or indirect harm to the client.
- Causation, foreseeability, damages to the patient, a duty that was owed to the client and this duty was breached, and a medical license.
Correct Response: B
The six essential components of malpractice include causation, foreseeability, damages to the patient, a duty that was owed to the client and this duty was breached, and, lastly, this breach of duty led to direct and/or indirect harm to the client.
A medical license is not necessary; nurses and other healthcare professionals can be found guilty of malpractice. Lastly, correlation is the relationship of simultaneously changing variables. For example, a ppositive correlation exists when the two variables both increase or decrease; and a negative occurs when one variable increases and the other decreases.
- Sound structures like policies and procedures
- Processes and how they are being done
- Optimal client outcomes
- Optimal staff performance
Correct Response: C
The current focus of performance improvement activities is to facilitate and address optimal client outcomes. Throughout the last several decades performance improvement activities have evolved from a focus on structures to a focus on process and now, to a focus on outcomes.
Staff performance is not the focus of performance improvement activities but instead the focus of competency assessment and validation.
- An adverse event
- A root cause
- A healthcare acquired event
- A sentinel event
Correct Response: D
A sentinel event is an event or occurrence, incident or accident that has led to or may have possibly led to client harm. Even near misses, that have the potential for harm, are considered sentinel events because they have the potential to cause harm in the future.
An adverse event, like an adverse effect of a medication, has actually led to an adverse response; it is not a near miss. A root cause is a factor that has led to a sentinel event; and there is no such thing as a healthcare acquired event.
- Discover a process flaw
- Determine who erred
- Discover environmental hazards
- Determine basic client needs
Correct Response: A
The primary purpose of root cause analysis is to discover process flaws. Root cause analysis and a blame free environment are essential to a successful performance improvement activity, therefore, root cause analysis does not aim to determine who erred and made a mistake. Root cause analysis explores and digs down to the roots of the problem, its root causes and the things, not people, which are the real reasons why medical errors and mistakes are made.
It is nursing assessment that determines the basic client needs and environmental surveillance that discovers environmental safety hazards, and not root cause analysis.
- What?
- Why?
- Who?
- When?
Correct Response: B
Root cause analysis activities ask “Why”, rather than “Who”, which would place blame on a person or group of people: and What? and When? Questions are rarely asked.
- Historical data and performance improvement activities focus on current data.
- Current data and performance improvement activities focus on historical data.
- Decreasing financial liability and performance improvement activities focus on process improvements.
- Decreasing falls and performance improvement activities focus on process improvements.
Correct Response: C
The primary distinguishing characteristic of risk management when compared and contrasted to performance improvement is that risk management activities focus on decreasing financial liability and performance improvement activities focus on process improvements.
Risk management focuses on decreasing and eliminating things that are risky and place the healthcare organization in a position of legal liability. Some examples of risk management activities include preventing hazards and adverse events such as patient falls and infant abduction and the legal liabilities associated with these events.
- Referrals complement the healthcare teams’ abilities to provide optimal care to the client.
- Referrals simply allow the client to be discharged into the community with the additional care they need.
- Nurses facilitate referrals to only the resources within the facility.
Correct Response: A
Referrals complement the healthcare teams’ abilities to provide optimal care to the client.
When clients have assessed needs that cannot be fulfilled and met by the registered nurse in collaboration with other members of the nursing care team, the registered nurse should then seek out resources, as well as utilize and employ different internal or external resources such as a physical therapist, a clergy member or a home health care agency in the community and external to the nurse’s healthcare agency.
The Safe & Effective Care Environment: Safety & Infection Control Practice Questions
- The sensitizing dose of penicillin can lead to anaphylaxis.
- The second dose of penicillin can lead to distributive shock.
- You should be aware of the fact that about 10% of the population has an allergy to both penicillin and latex.
- You should be aware of the fact that about 20% of the population has an allergy to both penicillin and latex.
Correct Response: B
The second dose of penicillin can lead to anaphylactic shock which is a form of distributive shock.
The first exposure to penicillin, referred to as the “sensitizing dose”, sensitizes and prepares the body to respond to a second exposure or dose. It is then the second exposure or dose that leads to anaphylaxis, or anaphylactic shock.
It is estimated that approximately 10% of people have had a reaction to penicillin. Some of these reactions are an allergic response and others are simply a troublesome side effect. There is no scientific data that indicates that 10% or 20% of the population has an allergy to both penicillin and latex.
- A 77 year old female client in a client room that has low glare floors.
- An 87 year old female client in a client room that has low glare floors.
- A 27 year old sedated male client.
- A 37 year old male client with impaired renal perfusion.
Correct Response: C
The 27 year old sedated male client is at greatest risk for falls.
Some of the risk factors associated with falls are sedating medications, high glare, not low glare, floors and other environmental factors such as clutter and scatter rugs, not low glare floors, a history of prior falls, a fear of falling, incontinence, confusion, sensory deficits, a decreased level of consciousness, impaired reaction time, advancing age, poor muscular strength, balance, coordination, gait and range of motion and some physical disorders, particularly those that affect the musculoskeletal or neurological systems; falls are not associated with poor and impaired renal perfusion.
- The nurse should advise clients in a smoke filled room to open the windows.
- The first thing that the nurse should do when using a fire extinguisher to put out a small fire is to aim the fire extinguisher at the base of the fire.
- Rapidly lift and move a client away from the source of the fire when their slippers are on fire.
- The home health care nurse should advise the client that the best fire extinguisher to have in the home is an ABC fire extinguisher.
Correct Response: D
The home health care nurse should advise the client that the best fire extinguisher to have in the home is an ABC fire extinguisher because this one fire extinguisher is a combination of a type A fire extinguisher, a type B and a type C, which put out all types of fires including common household solids like wood, household oils like kitchen grease and electrical fires.
The nurse should advise the client GET LOW AND GO if a room fills with smoke. They should not take any time to open window.
The first thing to do when using a fire extinguisher is to pull the pin and then aim it at the base of the fire. Later, you would squeeze the trigger and sweep the spray over and over again over the base of the fire. The acronym PASS is used to remember these sequential steps.
When a person has clothing that has caught on fire, the person should STOP, DROP AND ROLL. Tell the person, to STOP, DROP, and to not run, and as you also cover the person with a blanket to smother the fire.
- A tornado that has touched down on the healthcare facility
- A severe cyclone that has destroyed nearby homes
- A massive train accident that brings victims to your facility
- An act of bioterrorism in a nearby factory
Correct Response: A
A tornado that has touched down on the healthcare facility is an example of an internal disaster because this tornado has directly affected the healthcare facility. Tornados, cyclones, hurricanes and other severe weather emergencies can be both an internal disaster when they affect the healthcare facility and also an external disaster when they impact on the lives of those living in the community. Hurricane Katrina is a good example of a weather emergency that affected not only healthcare facilities but also members of the community.
- Use a slide board.
- Use a mechanical lift.
- Use a gait belt.
- Notify the client's doctor that the client cannot be safely transferred by you.
Correct Response: B
The best and safest way to transfer this paralyzed client when you suspect that you will need the help of another for the client’s first transfer out of bed is to use a mechanical lift. It is not necessary or appropriate to notify the doctor.
Mechanical lifts are used mostly for patients who are obese and cannot be safely moved or transferred by two people, and also for patients who are, for one reason or another, not able to provide any help or assistance with their lifts and transfers, such as a person who is paralyzed.
A gait or transfer belt and slide boards are assistive devices that can be used to assist with transfers and lifting however, they are not appropriate for this client as based on your assessment.
- Advise the nurse that the legs must be close together for stability during lifting and transfers.
- Advise the nurse that the legs should be one in front of the other and not spread apart during a transfer.
- Validate the nurse’s competency in terms of the application of body mechanics principles during a transfer.
- Validate the nurse’s competency in terms of the application of ergonomics principles during a transfer.
Correct Response: C
You should validate the nurse’s competency in terms of the application of body mechanics principles during a transfer because the nurse had spread her legs apart during the transfer to provide a wide base of support, which is a basic principle of body mechanics and not ergonomics.
Simply defined ergonomics addresses correct bodily alignment such as the lumbar curve accommodation in an ergonomically designed chair; and body mechanics is the safe use of the body using the correct posture, bodily alignment, balance and bodily movements to safely bend, carry, lift and move objects and people.
- The client has refrigerated foods labelled with an expiration date.
- You assess that the home is free of scatter rugs that many use to protect the feet against hard floors.
- The client uses the FIFO method for insuring food safety.
- The client assures you that the smoke alarm batteries are replaced annually to insure that they work.
Correct Response: D
When the client assures the nurse that they replace their smoke alarm batteries annually to insure that they work, the assessing nurse should immediately know that the client is in need of education relating to the fact that smoke alarm batteries should be changed at least twice a year.
The client has demonstrated that they are knowledgeable about food safety and environmental safety because they have expiration dates on refrigerated foods, they use the FIFO method for food safety and they do not use scatter rugs which can lead to falls.
The FIFO rule is First In is First Out. In other words, the first foods in the pantry or refrigerator are the first foods that should be consumed or discarded.
- It is clear?
- It is damaging to the lungs.
- It is damaging to the spleen and the liver.
- It leads to the over production of hemoglobin.
Correct Response: A
Carbon monoxide is particularly dangerous because it is clear, invisible and odorless. Carbon monoxide poisoning can occur when a person is exposed to an excessive amount of this odorless and colorless gas; it severely impairs the body to absorb life sustaining oxygen which is the result of this deadly gas and not damage to the lungs. This oxygen absorption deficit can lead to serious tissue damage and death. For these reasons, home carbon monoxide alarms are recommended.
These dangers are associated with deoxygenation and not splenic or hepatic damage or the over production of hemoglobin.
- Sentinel event.
- System variance.
- Adverse effect.
- Provider variance.
Correct Response: B
The lack of necessary supplies and equipment to adequately and safely care for patients is an example of a system variance.
A variance is defined as a deviation that leads to a quality defect or problem. Variances can be classified as a practitioner variance, a system/institutional variance, a patient variance, a random variance and a specific variance.
A sentinel event is defined as is an event or occurrence, incident or accident that has led to or may possibly lead to client harm. Adverse effects are serious and unanticipated responses to interventions and treatments, including things like medications.
- Notify the doctor.
- Render care.
- Assess the cleint.
- Notify the nurse manager.
Correct Response: C
The first thing that you should do immediately after a client accident is to assess the client and the second thing you should do is render care after this assessment and not before it.
Lastly, notifications to the doctor and the nurse manager are only done after the client is assessed and emergency care, if any, is rendered.
- Counsel the staff about their need to stop wasting the resources of this department.
- Check the equipment yourself to determine the accuracy of this equipment department.
- Ignore it because everyone can make an innocent mistake.
- Plan an educational activity about determining what equipment to send for repairs.
Correct Response: D
You should plan an educational activity about determining what equipment should and should not be sent for repairs. This data suggests that the staff members need education and training about the proper functioning of equipment used on the nursing care unit.
Counseling the staff about their need to stop wasting the resources of this department is placing blame and this blame may prevent future valid returns of equipment.
You should not check the equipment yourself to determine the accuracy of this equipment department because they are the experts, not you, with these matters.
You should also not ignore it because everyone can make an innocent mistake. The issue has to be addressed and corrected.
- Education and training on all pieces of equipment
- Pilot testing new equipment
- Reading all the manufacturer’s instructions
- Researching the equipment before recommending its purchase
Correct Response: A
Education and training on all pieces of equipment is an essential component for insuring that medical equipment is being used safely and properly by those who you supervise. Other essential components include validated and documented competency to use any and all pieces of equipment by a person qualified to do so, preventive maintenance and the prompt removal of all unsafe equipment from service.
Pilot testing new equipment, researching the equipment before recommending its purchase, and reading the entire manufacturer’s instructions are things done prior to the purchase of the equipment and these things do not impact on the safety of the piece of medical equipment.
- A possible vulnerability of the facility’s information technology to hacking
- The assisted suicide of a client in your facility by the spouse of the client
- Vulnerability to computer hacking
- Potential information theft
Correct Response: B
The assisted suicide of a client in your facility by the spouse of the client is a security concern that is also a sentinel event that must be reported.
A possible vulnerability of the facility’s information technology to hacking, vulnerability to computer hacking and potential information theft is security concerns but they are not sentinel events that must be reported.
- Training all nurses to serve as a part of a security response team
- Training all clerical staff to be a part of a security response team
- The restriction of visitors in a special care area
- Bar coded client identification bands to insure proper identification
Correct Response: C
The restriction of visitors in a special care area is an effective security plan that you may want to consider for implementation within your facility.
Some of the other security measures that you may want to consider include security alert systems to alert staff to a security breach such as security breach of the newborn nursery, the use of visitor identification badges or stickers that identify people who are authorized to be in a facility, closed circuit monitoring and alarm systems in high risk areas such as the emergency care area, automatically locking security doors, and electronic wristbands for the newborn and the mother to prevent infant abductions.
Special assignments and training for a group of people so that this specially trained group can act when a security breach occurs is also a good idea but it is not necessary to train all nurses or clerical staff; it is sufficient to train a limited group of people, provided an ample number of these team members are assigned and available on all tours of duty around the clock, including on holidays.
- Sterile items ONLY are placed on the sterile field.
- The nurse must keep the sterile field below waist level.
- Coughing or sneezing over the sterile field contaminates the sterile field.
- The nurse must maintain a 1/2 inch border around the sterile field that is not sterile.
- Moisture and wetness contaminate the sterile field.
- Sterile masks are used by staff and the client when a sterile field is being set up and/or maintained
Correct Response: A, C, E
Sterile items ONLY are placed on the sterile field; coughing or sneezing over the sterile field contaminates the sterile field; and all moisture and wetness contaminate the sterile field.
Some of the other principles that are applied to setting up and maintaining a sterile field include keeping the sterile field above the waist level and preventing coughing or sneezing by professional staff and the client during the set up and during the maintenance of the sterile field. If there is a danger that anyone may cough or sneeze over the field, the professional staff and/or the client should don a mask to prevent contamination. Lastly, a one inch border, not a ½ border that is not sterile is maintained around the perimeter of the sterile field.
- A physical restraint: A physical restraint is a manufactured device that is used, when necessary, to prevent falls.
- A physical restraint: A physical restraint is any mechanical device, material, or equipment attached to or adjacent to the resident’s body that the individual cannot remove easily which restricts freedom of movement or normal access to one’s body.
- A chemical restraint: A chemical restraint is a drug used for sedation to prevent falls.
- A chemical restraint: A chemical restraint is a drug used for discipline or convenience and not required to treat medical symptoms.
Correct Response: D
A chemical restraint: A chemical restraint is a drug used for discipline or convenience and not required to treat medical symptoms, according to the Centers for Medicare and Medicaid Services.
The most complete and accurate definition of a physical restraint is any manual method or physical or mechanical device, material, or equipment attached to or adjacent to the resident’s body that the individual cannot remove easily which restricts freedom of movement or normal access to one’s body and is NOT a safety devices that is routinely used for certain procedures, according to the Centers for Medicare and Medicaid Services.
- Informed consent for the restraint
- The reason for the restraint
- The type of restraint to be used
- Client behaviors that necessitated the restraints
Correct Response: A
The minimal components of orders for restraint include the reason for and rationale for the use of the restraint, the type of restraint to be used, how long the restraint can be used, the client behaviors that necessitated the use of the restraints, and any special instructions beyond and above those required by the facility’s policies and procedures.
Informed consent is not necessary for the initiation or the use of restraints
- The vascular phase
- The prodromal phase
- The incubation phase
- The initial injury
- The exudate phase
- The convalescence phase
- 4,2,1
- 4,1,5
- 4,5,1
- 4,2,5
Correct Response: B
The stages of the inflammatory process in correct sequential order are:
- The initial tissue injury which can result from an infection or a traumatic cause
- The vascular response. The release of histamine, prostaglandins and kinins. These substances lead to vasodilation which increases the necessary blood supply to the injured tissue and the area surrounding
- The exudate response. The release of leukocytes, including macrophages and neutrophils, to the injured area to combat the infection.
The signs of infection such as the incubation, prodromal and convalescence stages, in the correct sequential order are:
- The incubation period
- The prodromal phase
- The illness stage
- The convalescence stage
Health Promotion & Maintenance Practice Questions
- The infant had doubled their birth weight at twelve months.
- The infant had tripled their birth weight at twelve months.
- The mother reports that the infant is drinking 60 mLs per kilogram of its body weight.
- The infant had grown ¼ inch since last month.
Correct Response: A
The normal assessment data for the infant at 12 months of age is that the infant has doubled their birth weight at 12 months of age.
The mother’s reports that the infant is drinking 60 mLs per kilogram of its body weight and the fact that the infant had grown ¼ inch since last month are not normal assessment data. Infants are fed breast milk or formula every two to four hours with a total daily intake of 80 to 100 mLs per kilogram of body weight.
As the neonate grows, they gain five to seven ounces during the first six months and then they double their birth weight during the first year; the head circumference increases a half inch each month for six months and then two tenths of an inch until the infant is one year of age. Similarly, the height or length of the newborn increases an inch a month for the first 6 months and then 1/2 inch a month until the infant is 1 year of age.
- The Programmed Longevity Theory
- The Immunological Theory of Aging
- The Endocrine Theory
- The Rate of Living Theory
Correct Response: B
The theory of aging that supports your belief that strict infection control prevention measures are necessary is the Immunological Theory of Aging. The Immunological Theory of Aging states that aging leads to the decline of the person’s defensive immune system and the decreased ability of the antibodies to protect us against infection.
The Programmed Longevity Theory of aging states that genetic instability and changes occur such as some genes turning on and off lead to the aging process; the Endocrine Theory of aging states that aging results from hormonal changes and the biological clock’s ticking; and Rate of Living Theory states that one’s longevity is the result of one’s rate of oxygen basal metabolism.
Other theories of aging are:
- Wear and Tear Theory: This theory describes aging as a function of the simple wearing out of the tissues and cells as one ages.
- Cross Linking Theory: This theory of aging explains that aging results for cell damage and disease from cross linked proteins in the body.
- Free Radicals Theory: This theory is based on the belief that free radicals in the body lead to cellular damage and the eventual cessation of organ functioning.
- Somatic DNA Damage Theory: Somatic DNA Damage theory is based on the belief that aging and death eventually occur because DNA damage, as continuously occurs in the human cells, continues to the point where they can no longer be repaired and replaced and, as a result, they accumulate in the body.
- Increased creatinine clearance.
- Impaired immune system.
- Decreased hepatic metabolism.
- Increased bodily fat.
Correct Response: C
The elderly population is at risk for more side effects, adverse drug reactions, and toxicity and over dosages of medications because the elderly have a decrease in terms of their hepatic metabolism secondary to the hepatic functioning changes of the elderly secondary to a decreased hepatic blood flow and functioning.
The elderly have decreased rather than increased creatinine clearance; the immune system is also decreased in terms of its functioning, however, this change impacts on the elderly’s ability to resist infection rather than impacting a medication’s side effects, adverse drug reactions, toxicity and over dosages; and, lastly, a decrease in terms of bodily fat, rather than an increase in terms of bodily fat impacts on medications. The distribution of drugs is impaired by decreases in the amount of body water, body fat and serum albumin; drug absorption is decreased with the aged patient’s increases in gastric acid pH and decreases in the surface area of the small intestine which absorbs medications and food nutrients.
- 7/7/2017
- 8/7/2017
- 6/7/2017
- 8/1/2017
Correct Response: A
The expected date of delivery is calculated using Nagle’s rule which is:
The first day of last menstrual period – 3 months + 7 days = the estimated date of delivery
For example, when the first day of the last menstrual period is 10/20/2016 you would:
- Subtract three months from 10/20/2016 and then you get 7/20/2016 and then
- Add seven days to 7/20/2016 and then get 7/27/2016, after which you would
- Add one year to 7/27/2016 to get the estimated date of delivery for7/27 of the following year which is 7/27/2017.
- You should explain that fetal lie is where the fetus’ presenting part is within the birth canal during labor, among other information about the other assessments.
- You should explain that fetal presentation is the relationship of the fetus’s spine to the mother’s spine, among other information about the other assessments.
- You should explain that fetal attitude is the relationship of the fetus’ presenting part to the anterior, posterior, right or left side of the mother’s pelvis, among other information about the other assessments.
- You should explain that fetal station is the level of the fetus’ presenting part in relationship to the mother’s ischial spines, among other information about the other assessments.
Correct Response: D
You should explain that fetal station is the level of the fetus’ presenting part in relationship to the mother’s ischial spines. Fetal station is measured in terms of the number of centimeters above or below the mother’s ischial spines. Fetal station is -1 to -5 when the fetus is from 1 to 5 centimeters above the ischial spines and it is from +1 to +5 when the fetus is from 1 to 5 centimeters below the level of the maternal ischial spines.
Fetal lie is defined as the relationship of the fetus’s spine to the mother’s spine. Fetal lie can a longitudinal, transverse or oblique life. Longitudinal lie, the most common and normal lie, occurs when the fetus’ spine is aligned with the mother’s spine in an up and down manner; a transverse lie occurs when the fetus’ spine is at a right ninety degree angle with the maternal spine; and, lastly, an oblique lie occurs when the fetus’ spine is diagonal to the mother’s spine.
Fetal presentation is defined by where the fetus’ presenting part is within the birth canal during labor. The possible fetal presentations are the cephalic presentation, the cephalic vertex presentation, the cephalic sinciput presentation, the cephalic face presentation, the cephalic brow presentation, the breech presentation, the complete breech presentation, the frank breech presentation, the shoulder breech presentation, and the footling presentation.
Fetal attitude is the positioning of the fetus’s body parts in relationship to each other. The normal attitude is general flexion in the “fetal position”. All attitudes, other than the normal attitude, can lead to a more intense and prolonged labor.
Fetal position is the relationship of the fetus’ presenting part to the anterior, posterior, right or left side of the mother’s pelvis.
- You should apply the principles of initiative when caring for preschool children.
- You should apply the principles of sensorimotor thought when caring for preschool children.
- You should apply the principles of intimacy when caring for the adolescent.
- You should apply the principles of concrete operations when caring for the adolescent.
Correct Response: A
You should apply the principles of initiative when caring for preschool children. The developmental task for preschool children is initiative, according to Eric Erickson.
The other developmental tasks, according to Eric Erickson are:
- Infant: Trust
- Toddler: Autonomy
- School Age Child: Industry
- Adolescent: Identity formation
- Young Adult: Intimacy
- Middle Aged Adult: Generativity
- Older Adults: Ego integrity
In the correct sequential order, Jean Piaget’s levels of cognitive development include:
- Sensorimotor thought: Infancy to About 2 Years of Age
- Preoperational and symbolic functioning: From 2 to 7 Years of Age
- Concrete operations: 7 to 11 Years of Age
- Formal operations: 12 Years of Age
- Pregnancy
- Puberty
- Childhood immunizations
- Separation anxiety
Correct Response: B
The expected life transition should you apply into your practice for these pediatric clients as you are caring for pediatric clients of all ages is puberty.
Throughout the life span, there are several significant expected life transitions that require the person to cope and adjust. Some of these expected life transitions include puberty, maternal and paternal attachments and bonding to the neonate, pregnancy, care of the newborn, parenting, and retirement.
Although young children will experience separation anxiety and they will also be maintained on an immunization schedule, these are not expected life changes.
- The Biophysical Dimension
- The Psychological and Emotional Dimension
- The Spiritual Dimension
- The Health Systems Dimension
Correct Response: C
The Dimensions Model of Health includes six dimensions that impact on the client, including the community. The Spiritual Dimension is not one of these six dimensions.
These dimensions are the:
- Biophysical Dimension
- Psychological and Emotional Dimension
- Health Systems Dimension
- Behavioral Dimension
- Socio-Cultural Dimension
- Physical Environment Dimension
- Mediterranean ethnicity for cystic fibrosis.
- African American ethnicity for Tay Sachs disease.
- British Isles ethnicity for psychiatric mental health disorders.
- Saudi Arabian ethnicity for sickle cell anemia.
Correct Response: D
You would identify a client who is of Saudi Arabian ethnicity for sickle cell anemia. Other ethnicities at greatest risk for sickle cell anemia include those who are African, Latin Americans, Southern Europeans and some clients from some Mediterranean nations.
Other disorders and diseases and the ethnicities associated with them are listed below
- Thalassemia: Clients with a Mediterranean ethnicity
- Tay Sachs Disease: Ashkenazi Jewish people
- Cystic Fibrosis: Clients with a European ethnicity
- Psychiatric Mental Health Disorders: African Americans and Native Americans
- Hypertension: African Americans, Pacific Islanders , Native Americans, Alaskan natives, Hispanic and Caribbean clients
- Diabetes: African Americans, Caribbeans, Native Americans and clients from India, Pakistan and Bangladesh
- Cancer: Caucasians and clients from Scotland and Ireland
- The need for a targeted assessment is based on the application of the nurse’s knowledge of pathophysiology and the presenting symptoms.
- The need for a targeted assessment is based on the application of the nurse’s knowledge of developmental needs and developmental delays.
- Targeted assessment is done on an annual basis for existing clients rather than a complete assessment that is done for new clients.
- Targeted assessments consist of a brief medical history and a complete assessment consists of a complete health history and a complete physical assessment.
Correct Response: A
The need for a targeted assessment is based on the application of the nurse’s knowledge of pathophysiology and the presenting symptoms. Targeted assessments and screenings are done in addition to routine and recommended screenings when a particular disorder has a genetic pathophysiological component for risk and when a client is presenting with a particular sign or symptom.
For example, a targeted assessments relating to nutritional status may be indicated when an infant or young child is listless and not gaining weight according the established criteria; an adolescent may be target screened for visual acuity when a high school teacher reports that the teen does not seem to be able to read things on the blackboard; and a toddler may be target screened when the parent reports that the child is not responding to their name.
- Genetic predisposition
- Lifestyle choices
- High risk behaviors
- An external locus of control
Correct Response: B
Life style choices are the risk factors that are most likely able to be corrected. Poor life style choices place a person at risk and they are often considered also risky behaviors.
As discussed before, some risks are preventable and correctable and others are not. For example, genetics, age and gender are NOT modifiable risks, but the risks associated with life style choices are modifiable, correctable and able to be eliminated when the person changes their behavior in reference to these risky behaviors.
Some risky life style choices include:
- Excessive sun exposure
- The lack of regular exercise
- A poor diet
- Cigarette smoking and the use of other tobacco products
- Alcohol use
- Illicit drug use
- Unprotected sex
- Avocational and hobby choices such as rock climbing
- Inadequate sleep and rest
Genetic predisposition is an innate and not correctable risk factor and an external locus of control can lead to poor life style choices, however, this is not the most likely correctable risk factor.
- A transdermal contraceptive patch
- A diaphragm
- A vaginal contraceptive ring
- None of the above
Correct Response: D
You would not recommend any of the above methods of contraception for this family.
You would not recommend the use of a transdermal contraceptive patch or a vaginal contraceptive ring for the couple because both of these contraceptive methods are contraindicated when the woman has a history of deep vein thrombosis and cigarette smoking; and you would also not recommend a diaphragm because the compliance of this couple cannot trusted because the couple has a history of the lack of adherence to medical regimens.
- Information about the lack of scientific evidence regarding the effectiveness of all herbs.
- Data to support the fact that magnets can be effective in terms of fibromyalgia pain, and as such, may be a good choice for this client.
- Research that suggests that prayer is an effective alternative method to relieve pain and stress that can be helpful to this client.
- Information that contraindicates the use of biofeedback because this alternative, complementary health practice can interfere with the client’s pacemaker functioning.
Correct Response: C
Scientific data now indicates that prayer is effective for the relief of stress, anxiety and pain, and as such, may be helpful to this client.
Some herbs, minerals and supplements are scientifically deemed as safe and effective and others are not scientifically effective and they can also lead to harm; at the current time, the National Institutes of Health (NIH) states that magnets are not scientifically effective and they are also not considered safe for clients with a pacemaker or insulin pump because these internally implanted devices can be adversely affected by the magnetic force of the magnet; and, lastly, biofeedback does not interfere with the client’s pacemaker functioning.
- A social worker
- A physical therapist
- An occupational therapist
- A speech therapist
Correct Response: A
The healthcare professional would you most likely refer this family to in order to address this deficit in terms of their instrumental activities of daily living (ADLs) is a social worker.
The activities of daily living are differentiated in terms of the basic activities of daily living and the instrumental activities of daily living. Examples of basic activities of daily living include things like bathing, mobility, ambulation, toileting, personal care and hygiene, grooming, dressing, and eating. Deficits in terms of the basic activities of daily living are best addressed by a physical and/or occupational therapist.
The instrumental activities of daily living are more advanced than the basic activities of daily living. The instrumental activities of daily living include things like grocery shopping, housework, meal preparation, the communication with others using something like a telephone, and having transportation. Deficits in terms of the instrumental activities of daily living are best addressed by a social worker. For example, the social worker may assist the client in terms of their transportation and they can also teach the client about how to grocery shop, for example.
- Olfactory Cranial Nerve: The sensory nerve that transmits the sense of smell to the olfactory foramina of the nose
- Optic Cranial Nerve: This sensory nerve transmits the sense of vision from the retina to the brain.
- Oculomotor Cranial Nerve: This motor and sensory nerve controls eye movements and visual acuity.
- Trochlear Cranial Nerve: This motor nerve innervates eye ball movement and the superior oblique muscle of the eyes.
- Abducens Cranial Nerve: This motor nerve innervates and controls the abduction of the eye using the lateral rectus muscle.
- Facial Cranial Nerve: This motor nerve controls facial movements, some salivary glands and gustatory sensations from the anterior part of the tongue.
- Glossopharyngeal Cranial Nerve: This sensory nerve This nerve gives us the sense of taste from the posterior tongue, and it also innervates the parotid glands
Correct Response: A,B,D,E
The olfactory cranial nerve is a sensory nerve that transmits the sense of smell to the olfactory foramina of the nose; the optic cranial nerve is also a sensory nerve and it transmits the sense of vision from the retina to the brain.
The trochlear cranial nerve is a motor nerve that innervates eye ball movement and the superior oblique muscle of the eyes; and the abducens cranial nerve is a motor nerve that innervates and controls the abduction of the eye using the lateral rectus muscle.
The oculomotor cranial nerve is a motor nerve controls eye movements, the sphincter of the pupils and the ciliary body muscles; it has no sensory function. The facial cranial nerve is a motor and sensory nerve which controls facial movements, some salivary glands and gustatory sensations from the anterior part of the tongue. And, lastly, the glossopharyngeal cranial nerve is both a motor and sensory nerve that gives us the sense of taste from the posterior tongue, and it also innervates the parotid glands.
- The Taylor test
- The Rinne test
- The Babinski test
- The APGAR test
Correct Response: B
The sense of hearing is assessed using the Rinne test and the Weber test and a tuning fork.
A Taylor hammer, not a Taylor test, is used to check reflexes like the biceps and triceps reflexes; the Babinski sign occurs when the foot goes into dorsiflexion and the great toe curls up; this sign is an abnormal response to this stimulation and it can indicate the presence of deep vein thrombosis. And lastly, the APGAR test is used to assess the neonate immediately after birth in terms of the infant’s appearance, grimace and reflexes, appearance in terms of skin color, and respiratory rate and effort.
- Inspection
- Light palpation
- Deep palpation
- Percussion
Correct Response: C
Deep palpation is cautiously done after light palpation when necessary because the client’s responses to deep palpation may include their tightening of the abdominal muscles, for example, which will make the light palpation less effective for this assessment, particularly if an area of pain or tenderness has been palpated.
Inspection is typically the first step and percussion of the abdomen should be done prior to any palpation, particularly deep palpation.
- Resonance
- Flatness
- Tympany
- Dullness
Correct Response:
The five types of sounds that are elicited during percussion are flatness, resonance, hyperresonance, tympany and dullness. Dullness is heard when percussion is done over a solid organ like the liver and spleen.
Flatness is normally assessed over muscles and bones; resonance is a hollow sound that is heard, for example, over the air filled lungs; and hyperresonance, which is a booming sound that is heard over abnormal lung tissue, as occurs among clients with chronic obstructive pulmonary disease (COPD); and, lastly, tympany is heard over the stomach with air as a drum like sound.
- A complete medical history, a general survey and a complete physical assessment.
- A complete medical history, a general survey and a focused physical assessment.
- A client interview, a significant other interview, a general survey and a complete physical assessment.
- A client interview, a significant other interview, a general survey and a focused physical assessment.
Correct Response: A
A comprehensive health assessment includes a complete medical history, a general survey and a complete physical assessment.
Although a complete medical history is done using a client interview and a significant other interview for much data, it is the health history and not the interview that is part of the comprehensive health assessment. A focused assessment is done as based on some pathology, sign or symptom and it is not considered a part of a comprehensive health assessment.
- Tympany: A hollow sound
- Dullness: A thud like sound
- Dullness: A hollow sound
- Resonance: A booming sound
Correct Response: B
Dullness is a thud like sound and not a hollow sound. Tympany is a drum like sound; and resonance is a hollow sound.
Psychosocial Integrity Practice Questions
- A couple which consists of a husband and wife both of whom are affected with Alzheimer’s disease
- A poverty stricken couple without any healthcare resources in the community
- A pregnant woman and a husband who was physically abused as a young child
- A wealthy couple with feelings that they are immune from punishment and above the law
Correct Response: C
A pregnant woman and a husband who was physically abused as a young child is the couple is at most risk for domestic violence because pregnancy and a personal prior history of abuse are two commonly occurring risk factors among abused woman and male abusers, respectively.
Current research indicates that abuse and neglect affect all people of all ages and of all socioeconomic classes including the wealthy as well as the poverty stricken.
Other patient populations at risk of abuse and neglect include female gender, infants, children, the cognitively impaired, the developmentally challenged, the elderly and those with physical or mental disabilities; some of the other traits and characteristics associated with abusers include substance related use and abuse, a psychiatric mental health disorder, poor parenting skills, poor anger management skills, poor self-esteem, poor coping skills, poor impulse control, immaturity, and the presence of a current crisis.
- Restrain the client
- Place the client in seclusion
- Get an order for a sedating medication
- Establish trust with the client.
Correct Response: D
The first thing that you should do to prevent violence towards others is to establish trust with the client. The first step in the nurse-client relationship is to establish trust in this therapeutic relationship. Without trust future collaboration, interventions and client outcomes cannot be accomplished to facilitate appropriate and safe behaviors.
Restraints and seclusion are not indicated until others are in imminent danger because of this client’s current violent behaviors and not a history of it. Lastly, sedating medications to prevent violence are also not the first things that are done.
- Psychological dependence secondary to amphetamine use
- Substance abuse secondary to amphetamine use
- Addiction secondary to amphetamine use
- Physical dependence secondary to amphetamine use
Correct Response: A
The appropriate nursing diagnosis for this client is “Psychological dependence secondary to amphetamine use”. Psychological dependence is defined as the person’s need to continue the use of the substance to avoid any unpleasant feelings and experiences that can occur when the substance is not taken. Amphetamines and hallucinogenic drugs like LSD are often associated with psychological dependence.
Substance abuse, simply defined, is one’s overindulgence of an addictive substance which can be alcohol, prescription drugs and/or illicit, illegal drugs. Substance abuse does not include prescribed medications, such as narcotic pain medications, that are being used for medical reasons; however, these same medications when used after there is no longer a medical need to use them is considered substance abuse.
Addiction is defined as the unending and constant need for the person to have the chosen substance even when the use of the substance causes the client to have serious physical, psychological, social and/or economic consequences and harm including a loss of control over the substance abuse and use. Contrary to popular opinion, addiction can occur with and without physical dependence.
Physical dependence occurs when the cessation of a drug causes adverse physical effects; these ill effects are typically greater and more intense when the cessation of the drug is rapid and abrupt. Some of the drugs that are most often associated with physical dependence include cocaine, opioid drugs, alcohol and benzodiazepines. As previously stated, physical dependence does not necessarily indicate addiction; addiction can be present with or without any physical dependency.
- Orem’s Self Care Model
- Nagi's Model
- A cognitive model of disability
- A biomedical model of disability
Correct Response: B
Nagi’s Model of disability model describes disabilities and its limitations are the result of a discrepancy between the client’s abilities and the limitations of the physical and social environment within which the client lives.
Although clients with disabilities should be assessed and have interventions related to their self care abilities, Dorothea Orem’s Self Care Model is not a model of disability. This model describes self care needs and abilities as wholly compensatory, partly compensatory and supportive educative.
Cognitive models of disability focus on the importance of affected client’s ability to remain as independent as possible and ways that the empowered client can exercise their own self-determination, confidence, self efficacy, and control.
Lastly, biomedical models address pathology, impairments and the manifestations of impairments that can be cured or lead to death.
- 3,2,1,4
- 1,2,3,4
- 4,3,2,1
- 4,3,1,2
Correct Response: D
The characteristics of the stages or phases of crisis, in the correct sequential order, are:
- Level 1 Crisis Signs and Symptoms: Patients experiencing a level one crisis typically experience anxiety and they also typically begin to use one or more psychological ego defense mechanisms.
- Level 2 Crisis Signs and Symptoms: Patients experiencing a level two crisis most likely exhibit some loss of their ability to function. They may also try to experiment with alternative methods of coping in order to deal with the crisis that is not being effectively coped with using one’s currently used coping mechanisms.
- Level 3 Crisis Signs and Symptoms: Patients experiencing a level three crisis show the signs and symptoms of the General Adaptation Syndrome which is characterized with fight, flight and panic as discussed above under the section entitled “Coping Mechanisms: Introduction”.
- Level 4 Crisis Signs and Symptoms: Clients experiencing a level four crisis exhibit severe signs and symptoms such as being totally detached and removed from others, feeling overwhelmed, becoming disoriented, and even with thoughts of violence toward self and others.
- Displacement
- Sublimation
- Dissociation
- Reaction formation
Correct Response: C
Dissociation is the psychological ego defense mechanism occurs when the client detaches and dissociates with person or time to avoid the stress until they are ready to cope with it.
Displacement transforms the target of one’s anger and hostility from one person to another person or object. Displacement allows the person to ventilate and act out on their anger in a less harmful and a more socially acceptable manner.
A client uses the ego defense mechanism of sublimation when they transform and replace unacceptable urges and feelings into a socially acceptable urge or feeling.
A client is using reaction formation when the client acts and behaves in a manner that is completely the polar opposite of their true feelings.
- Jean Watson's
- Martha Rogers'
- Nagi's theory
- Madeleine Leininger’s theory
Correct Response: D
The theoretical framework that you would recommend that this committee should consider when addressing mutiethnicity and the culturally diverse nature of this facility for this philosophy is Madeleine Leininger’s theory.
Madeleine Leininger’s theory of Transcultural Nursing and her book “Culture Care Diversity and Universality: A Theory of Nursing” “searches for comprehensive and holistic care data relying on social structure, worldview, and multiple factors in a culture in order to get a holistic knowledge base about care” (Leininger, 2006, p. 219)
Jean Watson’s Jean Watson developed the Human Caring Theory which states that caring is the essence of nursing. Watson's theory has the four major concepts of health, nursing, society/environment and human being. Caring consists of the following 10 nursing interventions that demonstrate genuine caring.
Martha Rogers’ theory is the Science of Unitary Human Beings which is based on general systems theory without any focus on multiethnicity and cultural diversity; and lastly, Nagi’s Model of disability model describes disabilities and its limitations are the result of a discrepancy between the client’s abilities and the limitations of the physical and social environment within which the client lives.
- The client will accept impending death
- Guilt related to past transgressions
- Spiritual distress related to guilt
- Pain related to end of life symptoms
Correct Response: A
“The client will accept impending death” is the client goal would be the most likely appropriate and expected for the vast majority of these clients. In fact, one of the primary goals of hospice and palliative care is to facilitate the client’s and family member’s acceptance.
Other goals are the freedom for guilt, spiritual distress and pain at the end of life; therefore, these diagnoses are not expected.
- The client will be free of constipation
- The client will remain free of pain and distress
- The administration of an antiemetic to prevent vomiting and further dehydration
- The administration of an enema to correct the constipation
Correct Response: B
Based on this client’s signs and symptoms and the fact that the client is expected to die in a day or two, the appropriate client outcome for this client is that the client will remain free of pain and distress.
“The client will be free of constipation” requires interventions such as an enema which are not indicated when death is imminent unless, of course, the client is adversely affected with pain and discomfort as the result of it which is not the case with this client. Additionally, the administration of an antiemetic to prevent vomiting is not indicated because there is no evidence in this question that the client is actually vomiting.
- “You should try to come to a few sessions at least because they may be very informative to you”.
- “You are probably correct. This really is not your problem”.
- “Despite the fact that it is your grandson’s drug addiction, situations such as this affect all members of the family including grandparents who live in the home.”
- "You should attend because the doctor has ordered family therapy for you as extended family members”.
Correct Response: C
You should respond to the grandparents’ statement with “Despite the fact that it is your grandson’s drug addiction, situations such as this affect all members of the family including grandparents who live in the home”.
After this statement, you should also educate the grandparents about the fact that group and family therapy is often indicated when the family unit is affected with stressors and dysfunction because family members may not fully understand the need for the entire family unit to participate when only one member of the family is adversely affected with a stressor and poor coping and that all family members are affected when only one member of the family unit is adversely affected.
You would NOT state “You should try to come to a few sessions at least because they may be very informative to you” because these sessions are therapeutic and not educational; you would not state “You are probably correct. This really is not your problem” because this statement is not true; and you should also not state “You should attend because the doctor has ordered family therapy for you as extended family members” because this is not the real reason why attending these sessions is needed.
- Engel's theory
- Kubler Ross' theory
- Lewin's theory
- Warden's theory
Correct Response: D
The theory of grief and loss would you most likely integrate into your practice as you perform this role is Warden’s Four Tasks of Mourning. This theory has four tasks that people go through after the loss of a loved one. These tasks are accepting the loss, coping with the loss, altering, modifying and changing the environment to cope with and accommodate for the absence of the lost person, and, finally, resuming one’s life while still having a healthy connection with the loved one.
Engel’s Stages of Grieving include stages both prior to and after a loss and these stages are:
- Shock and disbelief
- Developing awareness
- Restitution
- Resolving the loss
- Idealization
- Outcome
Kubler Ross’s Stages of Grieving occur prior to the death and these stages include:
- Denial
- Anger
- Bargaining
- Depression
- Acceptance
Lastly, Lewin developed theories of change, leadership and conflict and NOT a theory related to grief after the loss of a loved one.
- The concern related to the client’s cultural reluctance to report psychological symptoms because of some possible culturally based stigma associated with psychiatric mental health disorders
- Concerns revolving around the lack of financial and health insurance resources to pay for psychological care
- Concerns related to the compliance with psychological treatment regimens because of the client’s lack of social support systems
- The concern related to the culturally based client apathy about nursing care and nursing assessments
Correct Response: A
The concern related to the client’s cultural reluctance to report psychological symptoms because of some possible culturally based stigma associated with psychiatric mental health disorders which is a barrier to assessment because the client fears being stigmatized and rejected when divulging psychological data including anxiety and other symptoms.
The lack of financial and health insurance resources to pay for psychological care, the lack of social support systems, and the client’s apathy are barriers to psychological care but these factors are not a barrier to a psychological assessment and these factors are not cultural, but instead social and psychological.
- Cognitive psychotherapy
- Behavioral psychotherapy
- Cognitive behavioral psychotherapy
- Psychoanalysis
Correct Response: B
Behavioral psychotherapy is particularly useful among clients who are adversely affected with phobias, substance related disorders, and other addictive disorders. Some of the techniques that are used with behavioral therapy include operant conditioning as put forth by Skinner, aversion therapy, desensitization therapy, modeling and complementary and alternative stress management techniques.
Cognitive psychotherapy is most often used to treat clients, including groups of clients, with depression, eating disorders, anxiety, and anxiety disorders to facilitate the altering of the clients’ attitudes and perspectives relating to stressors.
Cognitive behavioral psychotherapy, which is a combination of cognitive psychotherapy and behavioral psychotherapy and also referred to as dialectical behavioral therapy is most often used for clients affected with a personality disorder and those at risk for injury and harm to self and/or others.
Psychoanalysis, in contrast to cognitive behavioral therapy and other individual and group therapies, dives into the client’s subconscious and it often focuses on the past as well as the client’s current issues. This therapy is not conducted by registered nurses but, instead, by experienced psychotherapists.
- Hinduism
- Buddhism
- Islam
- Mormonism
Correct Response: C
The client religion that is the most pertinent to the role of the admissions coordinator of hospital who assigns the rooms and beds of clients who will be admitted is the Islam religion which requires that the followers face Mecca for daily prayer, therefore, Islam clients should be placed in a room that faces the holy city of Mecca.
Although most religions impact on the care of the client, only Islam is pertinent to the admissions coordinator. Other religions practices and their impact on health care are shown below:
- Christians: End of life rituals like the Sacrament of the Sick, baptisms for newborns, fasting, and the Eucharist.
- Judaism: Religious based circumcisions, a kosher diet which separates dairy foods from meat based foods, and death rituals called a Shiva.
- Hinduism: Many followers are vegetarian; personal hygiene is paramount and they also have death rituals without the prolongation of life.
- Mormonism: Baptism for the newborn, last rites at the time of death, communion, and burials of the dead. Additionally, the Mormon religion prohibits alcohol, tobacco, and caffeine.
- Jehovah’s Witnesses: Prohibitions against blood transfusions, foods containing blood, homosexuality, sex before marriage, abortion, suicide, gambling, alcoholic beverages, tobacco and illicit drugs.
- Psychotic symptoms related to sensory overload
- Psychotic symptoms related to a previously undiagnosed psychosis
- Visual disturbances related to dementia
- Visual disturbances related to delirium
Correct Response: D
“Visual disturbances related to delirium” is the most appropriate nursing diagnosis for this client, as based on their signs, symptoms, past history and current medical status.
Delirium is characterized with a sudden and abrupt onset of episodic and intermittent periods of time vacillating between periods of impaired cognition and periods of mental clarity. Visual hallucinations are a sign of delirium and delirium can result from a number of different causes including dehydration and anticholinergic medications.
The signs and symptoms of sensory overload do not include visual hallucinations and a sudden and abrupt onset of episodic and intermittent periods of time vacillating between periods of impaired cognition and periods of mental clarity. Instead, the signs and symptoms of sensory overload include anxiety, restlessness, sleep deprivation, fatigue, poor problem solving and decision making skills, poor performance, and muscular tension.
There is no evidence in this question that the client has psychotic symptoms related to a previously undiagnosed psychosis; all the evidence substantiates the suspicion that the client is affected with delirium.
Lastly, dementia has a gradual and progressive onset rather than an abrupt and sudden onset.
- Collect baseline blood pressure readings prior to the beginning of this educational series and then collect and compare blood pressure data during the series and after the series is completed.
- Collect baseline blood pressure readings prior to the beginning of this educational series and then collect and compare blood pressure data after the series is completed.
- Ask the clients how often they use the stress management techniques that they have learned during this educational series.
- Use a questionnaire at the end of the series that asks the participants how they liked the class and what they learned during this educational series.
Correct Response: A
The best way to evaluate the effectiveness of this educational series is to collect baseline blood pressure readings prior to the beginning of this educational series and then collect and compare blood pressure data during the series and after the series is completed. This technique entails evaluating the outcomes of the education in terms of changes in the client and it also includes formative evaluation during the series and summative evaluation at the end of the series.
Collecting baseline blood pressure readings prior to the beginning of this educational series and then collecting and comparing blood pressure data after the series is completed gives us only summative evaluation; it does not provide you with formative evaluation.
Because the primary goal of this series is to lower the blood pressures of clients through the use of stress management techniques, asking the clients how often they use the stress management techniques that they have learned during this educational series and using a questionnaire at the end of the series that asks the participants how they liked the class and what they learned during this educational series does not reflect data and information about the effectiveness of the classes in terms of reducing the blood pressures of hypertensive clients.
- Reiki
- Tai Chi
- Feng Shui
- Jiu Jitsu
Correct Response: A
Tai Chi is a type of a mind body exercise that deeply focuses on breathing, movement and meditation. Yoga is similar to tai chi in that yoga also employs a combination of breathing, movement and meditation.
Reiki is done for the client when the therapist places their hands on or near the person’s body to promote the client’s energy field and its own natural healing processes. Feng shui is an eastern method of decorating using colors, items and the placement of objects in the environment to promote a harmonious relationship of man and its environment; and lastly Jiu Jitsu is a martial art.
- You should advise the couple to move closer to their children so that they can care for their father.
- You should teach the wife about this progressive disease and the need to promote as much independence as possible.
- You should teach the wife about this progressive disease and the need to do all that she can for the husband to avoid his depression and frustration.
- You should advise the couple to decrease their social activities in order to preserve the husband’s dignity and self-esteem.
Correct Response: B
You should teach the wife about this progressive disease and the need to promote as much independence as possible. Client’s with Alzheimer’s disease and other disabilities, including physical disabilities, should be coached and encouraged to be as independent as possible.
Moving closer to the children may not be appropriate advice particularly if the children are unable or unwilling to care for their father. Lastly, you should advise the couple to continue their social activities and to only avoid those situations where the necessary compassion and understanding about the client and his condition are absent.
- According to the Global Deterioration Scale, clients in the first stage of Alzheimer’s disease tend to cover up their failing abilities
- According to the Reisberg Scale, clients in the first stage of Alzheimer’s disease tend to cover up their failing abilities
- According to the Global Deterioration Scale, clients in the third stage of Alzheimer’s disease tend to cover up their failing abilities
- According to the Reisberg Scale, clients in the fourth stage of Alzheimer’s disease tend to cover up their failing abilities
Correct Response: C
According to the Global Deterioration Scale, also referred to as the Reisberg Scale, clients in the third stage of Alzheimer’s disease tend to cover up their failing abilities.
The Global Deterioration Scale stages Alzheimer’s according to seven stages. These stages include
- Stage 1: Cognitive abilities are intact.
- Stage 2: Minimal and hardly noticeable forgetfulness occurs.
- Stage 3: Mild changes in terms of cognition occur. The client may have difficulty in terms of their memory, which at times the client may “cover up” to avoid the detection by others. The signs and symptoms of this stage are similar to those of the Early Stage of Alzheimer’s disease, as discussed immediately above.
- Stage 4: This stage is characterized with increasing confusion about recent events and conversations, mild problems with math and some rather routinized sequential tasks such as cooking. The client may withdraw from others and debate the fact that they are having some cognitive issues.
- Stage 5: Early Dementia occurs. Short and long term memory losses, a lack of orientation to place and time, poor judgment, and some of the client’s self care in terms of the activities of daily living become progressively more problematic. The client may need the assistance and supervision of others to promote the client’s highest possible level of independence in the performance of their basic activities of daily living.
- Stage 6: This stage is referred to a Middle Dementia and moderately severe Alzheimer’s disease. There is almost complete short term and long term memory loss, communication is highly limited and it may only consist of nonverbal behavioral responses, and the client needs complete care to manage their activities of daily living. Sundowner’s syndrome is present and hallucinations as well as agitation may occur.
- Stage 7: This stage is referred to as Late or Severe Dementia and Failure to Thrive. The client is in need of complete care; and immobilization, in addition to the hazards of immobility, may affect the client and the family members at this stage.
- Probing for more information from the client
- Sublimation to determine hidden messages
- Providing privacy so the client is comfortable
- Silence to allow contemplation and thought
- A safe environment of care that is conducive to the prevention of medical errors.
- A client care area that provides personal privacy and the confidentiality of medical information.
- A European method of design and color to promote health and wellness.
- The provision of a therapeutic environment of consistency to promote health.
Correct Response: D
A therapeutic milieu eliminates as many stressors from the environment as possible. The goal of this environment is to facilitate the client’s coping and recovery without the need to cope with these extraneous and avoidable stressors. Some of the elements of a therapeutic milieu environment include consistency, client rules, limitations and boundaries, and client expectations, including contracts, relating to appropriate behavior.
Physiological Integrity: Basic Care & Comfort Practice Questions
- Psychomotor domain: The client will slightly bend their elbows when holding the hand grips.
- Psychomotor domain: The client will rest their weight on the padded areas on the top of the crutches.
- Cognitive domain: The client will slightly bend their elbows when holding the hand grips.
- Cognitive domain: The nurse will tell the client how often the tips on the crutches must be replaced.
Correct Response: A
The client goal that is paired with its learning domain that should be included in the patient teaching plan for this client and the parents is “The client will slightly bend their elbows when holding the hand grips” which is part of the psychomotor domain and not the cognitive domain. Lastly, the “nurse will” is an intervention and not a client goal or expected outcome which should be learner, not nurse, oriented.
- An aphasia aid
- A button hook
- Honey thickened liquids
- A word board
Correct Response: B
The basic activity of daily living assistive device can be useful for the client who is affected with poor fine motor coordination is a button hook that would be used for the dressing activity of daily living.
An aphasia aid and a word board are assistive devices to facilitate communication when the client is affected with a communication deficit such as aphasia; and, lastly honey thickened liquids are indicated for clients with a swallowing disorder and they are not indicated for clients with poor fine motor coordination.
- Place the client in a wheelchair to protect their safety in the clinic.
- Remove the cane from the client to protect their safety.
- Teach the client about the proper length of a cane.
- Have the client use a wheelchair rather than the cane.
Correct Response: C
You should teach the client about the proper length of a cane. The proper length of the cane should be the length that only permits the client’s elbow to be slightly flexed. Some canes like a wooden cane are not adjustable to the client’s height and others can be adjusted to meet the height needs of the client.
You would not place the client in a wheelchair or ask the client to use a wheelchair and you would also not take the cane, which is their personal property, away from them. You would use this observation as a learning need assessment and, as such, you should teach the client about the proper length of a cane and help them to adjust the height of the cane if the client’s cane is a height adjustable one.
- A cleansing enema
- A retention enema
- A return-flow enema
- A laxative
Correct Response: C
The most likely intervention for this client, after getting a doctor’s order, is a return flow enema. Return-flow enemas, similar to a carminative enema, are used to relieve flatus and stimulate peristalsis which is frequently a problem after a client has received anesthesia.
Cleansing enemas are used to relieve constipation; and a retention enema is used to administer a medication, to soften stool and to lubricate the rectum so that it is easier and more comfortable for the client to defecate.
Finally, the data in this question does not indicate that the client is constipated and in need of a laxative.
- Both can lead to infection.
- Both are invasive procedures.
- Both are considered sentinel.
- Both are the last resort.
Correct Response: D
The commonality that is shared in terms of both restraints and urinary catheters is that both are the last, not the first, treatment of choice. Both indwelling urinary catheters and restraints pose risks and complication; therefore, both of these interventions must be prevented with the use of preventive measures.
Indwelling urinary catheters are invasive but restraints are not invasive; indwelling urinary catheters can lead to infection but restraints do not. Lastly, neither are sentinel. A sentinel event is an event or occurrence, incident or accident that has led to or may have possibly led to client harm. Even near misses, that have the potential for harm, are considered sentinel events because they have the potential to cause harm in the future.
- Any solid skin barrier
- A hydrocolloid solid skin barrier
- Hollister’s Flextend
- A skin sealant
Correct Response: D
You would recommend a skin sealant, including products like Bard’s Protective Barrier and Convatec’s Allkare, which are a fast drying polymer transparent film that can be applied relatively simply with a wipe or a spray. These products are easy to use and less expensive than solid skin barriers, including Hollister’s Flextend and others containing hydrocolloids.
- A prolapsed stoma
- A vitamin B12 deficiency
- Nocturnal enuresis
- GI stone formation
Correct Response: A
Some of the complications associated with a colostomy include a prolapsed stoma, infection, dehiscence, an ischemic ileostomy, a peristomal hernia, stoma stenosis, stomal retraction, necrosis, mucocutaneous separation, stomal trauma, peristomal skin damage as the result of leakage and parastomal hernias.
A vitamin B12 deficiency, nocturnal enuresis and urinary stone formations are complications associated with urinary diversion and not fecal ostomy diversions.
- Bone demineralization: Turning and positioning every 2 hours
- Urinary stasis: The client will consume 1,000 mL of oral fluids per day
- Muscle atrophy: The client will perform range of motion exercises at least 3 times a day
- Hypercalcemia: Maintaining fluid intake of 1,000 mL per day
Correct Response: C
“The client will perform range of motion exercises at least 3 times a day” is an appropriate expected outcome of care that the nurse provides to prevent this complication.
Urinary stasis and hypercalcemia, both hazards of immobility, can be prevented when the client will consume 2,000 mL of oral fluids per day. Lastly, calcium loss from the bones can be prevented by weight bearing activity, and not turning and positioning in bed.
- 1 on the scale of 1 to 3
- 2 on the scale of 1 to 5
- 3 on the scale of 0 to 5
- 4 on the scale of 0 to 5
Correct Response: C
You would document this client’s muscular strength as a 3 on a scale of 0 to 5.
Muscular strength is classified on a scale of zero to five, as below.
- Zero: No muscular contraction
- One: No muscular movement, only a quiver is noted
- Two: Muscular movement but only when assisted with gravity
- Three: Muscular movement against gravity but not against resistance
- Four: Muscular movement against resistance
- Five: Full muscular movement and strength
- 6 cm
- 12 cm
- 20 cm
- 24 cm
Correct Response: D
You would document the size of this wound as 24 cm. After the wound is assessed and measured, the wound dimension is calculated by multiplying the length by the width by the depth of the wound. For example when the length of the sound is 3 cm deep, 2 cm long and 4 cm wide, it is calculated with 3 x 2 x 4 = 24 cm.
- Secondary intention healing
- Tertiary intention healing
- Primary prevention healing
- Secondary prevention healing
Correct Response: A
Secondary intention healing is the most likely type of wound healing for this client because of the risks associated with the deep infection associated with the ruptured appendix and the peritonitis.
Secondary intention healing, also referred to as healing by second intention, is done for contaminated wounds in order to prevent infections, to prevent the formation of abscesses and to promote healing from the bottom up to the outer surface of the skin so that any potential infection is not closed in at the bottom of the wound. These open wounds are irrigated with a sterile solution and then packed to keep them open and, over time, they will heal on their own. The resulting scar is more obvious than those scars that result from primary intention healing.
Primary intention healing is facilitated with wounds without infection. The wound edges are approximated and closed with a closure technique such as suturing, Steri Strips, and surgical glues.
Tertiary intention healing, also referred to as healing by tertiary intention, is a combination of secondary and primary healing. Tertiary intention healing begins with several days of open wound irrigations and packing, which is secondary healing, followed by the closure of the wound edges with approximation and suturing which is primary healing. Some traumatic wounds are healed with tertiary intention.
Primary, secondary and tertiary prevention strategies are prevention, interventions and restorative or rehabilitation care and not methods of wound healing.
- A barrier film
- An alginate dressing
- Surgical laser debridement
- Autolytic debridement
Correct Response: B
The treatment of pressure ulcers is complex and it often includes a combination of treatments and therapies. The RYB Color Code of Wounds is sometimes used by nurses to guide the treatment options. RYB stands for the colors of red, yellow and black. The rules of treatment for these three colors are:
- Red: Covering with a dressing such as a hydrocolloid film, turning and positioning the client and avoiding pressure, friction and shearing
- Yellow: Using an alginate dressing
- Black: Debridement, including surgical laser debridement, mechanical debridement, autolytic debridement, enzymatic debridement and sharp instrument debridement, of the area to remove the black necrotic eschar.
- Moritz Schiff’s theory of pain
- The Intensive Theory of Pain
- Melzack and Wall’s theory of pain
- The Specificity Theory of Pain
Correct Response: C
Melzack and Wall’s Gate Control Theory of pain supports the belief that some of the factors that open this “gate” to pain are low endorphins and anxiety and that some of the factors that close this “gate” to pain are decreased anxiety and fear. The substantia gelatinosa is the “gate” that facilitates or blocks the transmission of pain.
The Specificity Theory of Moritz Schiff described pain as a sensation that was different from all the other senses in that pain had its own specific nervous system pathways from the spinal cord that traveled to the brain; the Intensive Theory of pain is based on the belief that pain is an emotional state, rather than a sensory phenomenon; the Peripheral Pattern Theory of pain of Sinclair and Weddell describes pain as the result of an intense stimulus applied to the skin; and the Neuromatrix Theory of Pain supports the fact that pain is a dynamic and multidimensional process with physical, behavioral, perceptual, psychological and social responses and one that can only be described by the person who is experiencing it.
- Pain level, the quality of the pain, the region or area of the pain, the severity of the pain, and the pain triggers
- Precipitating factors, the quality of the pain, relief factors, the severity of the pain, and the pain triggers
- Pain level, the quantitative numerical pain score, the region or area of the pain, the severity of the pain, and the pain triggers
- Precipitating factors, the quality of the pain, the region or area of the pain, the severity of the pain, and the pain triggers
Correct Response: D
Precipitating factors, the quality of the pain, the region or area of the pain, the severity of the pain, and the pain triggers are the PQRSTs of the PQRST method of pain assessment.
The severity of the pain, which can include a quantitative, numerical pain score from 1 to 10, for example, is the S of the PQRST method of pain assessment.
- Assessment data, biochemical data, clinical data and dietary data
- Ancestral cultural data, biochemical data, clinical data and dietary data
- Anthropometric data, biological data, chemical data and dietary data
- Anthropometric data, biochemical data, clinical data and dietary data
Correct Response: D
Anthropometric data, biochemical data, clinical data and dietary data are the A, B, C and Ds of a complete and comprehensive nutritional assessment.
The elements of these A, B, C and Ds of nutritional assessment include:
- A: Anthropometric Data: This data includes variables such as height, weight, body mass index and arm measurements such as the mid arm circumference and the triceps skin fold.
- B: Biochemical Data: Laboratory testing data like serum albumin, hemoglobin, urinary creatinine, and serum transferrin.
- C: Clinical Data: The client’s skin condition, level of activity and status of the client’s mucous membranes.
- D: Dietary Data: This data includes the client’s subjective reports of their food and fluid intake over the last 24 hours and the types of foods that are typically eating.
- Constipation: The provision of a high fiber diet
- Urinary pH changes: Encouraging ample oral fluid intake
- Aspiration: Maintaining the client in at least a 30 degree angle
- Aspiration: Maintaining the client in at least a 90 degree angle
Correct Response: C
Aspiration can be prevented by maintaining the client in at least a 30 degree angle; a 90 degree angle is not only not necessary, this angle places a client at greater risk for the development of a pressure ulcer.
Diarrhea, rather than constipation is a complication of tube feedings; and urinary pH changes are not a commonly occurring complication of tube feedings.
Some of the other complications and preventive measures are:
- Diarrhea: Maintaining a slow rate of infusion whenever possible, changing the ordered rate and formula when necessary
- Abdominal pain: Maintaining a slow rate of infusion whenever possible
- Dehydration: Monitor the client for any signs and symptoms of dehydration, measure intake and output and notify the doctor of any abnormalities
- Nausea and Vomiting: Slowing the rate down, changing the formula and antiemetic medications to stop the vomiting and to prevent any aspiration
- Tube Dislodgment: Secure and monitor the tube
- Culture
- Locus of control
- Bodily surface area
- Diaphoresis
Correct Response: A
There are a wide variety of different factors that influence and impact on our clients’ hygiene habits and routines. For example, cultural practices and beliefs, ethnical factors, religious practices and beliefs, the client’s level of growth and development.
Although the locus of control, bodily surface area and diaphoresis in addition to other factors such as economic constraints, the client’s level of energy, the client’s level of cognition, and environmental factors can impact on hygiene, these are not factors that impact on the client’s hygiene and hygiene practices; they do not typically impact on the lifelong developed hygiene and hygiene practices.
- The neonate: 10 to 15 hours a day
- The toddler: 11 to 14 hours a day
- The preschool child: 12 to 15 hours a day
- The school age child: Less than 8 hours a day
Correct Response: B
The age group that is accurately paired with the normal and recommended hours of sleep each day is the toddler should sleep about 11 to 14 hours per day.
The neonate should sleep 14 to 17 hours per day; the preschool child should sleep 10 to 13 hours per day; and the school age child should sleep 9 to 11 hours per day.
Physiological Integrity: Pharmacological & Parenteral Therapies Practice Questions
- Stop the intravenous flow
- Slow down the intravenous flow
- Notify the doctor
- Begin CPR
Correct Response: A
Your first priority intervention is to immediately stop the flow of the intravenous antibiotic because it is highly likely that the signs of anaphylaxis have occurred as the result of the client’s adverse effect to this antibiotic.
The next thing that you would do is assess the client to determine their physical status and to provide necessary emergency measures, including CPR, if it is indicated. Later, you would notify the doctor about this adverse reaction.
- Mix a small amount of the medication in a small amount of the intravenous fluid and then examine this mixture for color changes
- Refer to a compatibility chart
- Call the doctor and ask if the medication is compatible with the particular intravenous fluid
- Mix a small amount of the medication in a small amount of the intravenous fluid and then examine this mixture for any precipitates
Correct Response: B
The best way to determine whether or not a medication is compatible for a particular intravenous fluid is to refer to a compatibility chart.
Although, at times, incompatibility can be evidenced with changes such as those related to color changes and the formation of a cloudy solution or obvious precipitate, at other times incompatibility may not be noticeable. For this reason, nurses must refer to a compatibility or incompatibility chart before they mix medications or medications and solutions.
Lastly, there is no need to call the doctor for compatibilities when you have, and should use, a compatibility chart.
- Prevent polypharmacy
- Conserve financial resources
- Prevent interactions
- Prevent allergies
Correct Response: C
The medication reconciliation process to insure that the nurse is aware of all medications that the client is taking, some of which may have been ordered by a physician other than the client’s primary care doctor and some of which are over the counter or alternative therapies that the client has added. The complete and current list of medications is then reviewed by the nurse and possible interactions are identified and addressed with the client.
Although this medication reconciliation process can also save costs by eliminating unnecessary medications, particularly when the client is taking multiple medications (polypharmacy), this is not a primary purpose. Lastly, medications that the client is allergic to should never be given, therefore, these medications should not appear during the medication reconciliation process; they should never have been given to or taken by the client.
- The fact that drugs classified as categories C, D and X are contraindicated for women who are pregnant.
- The fact that drugs classified as categories A, B and C are contraindicated for women who are pregnant.
- The fact that drugs classified as categories C, D and E are contraindicated for women who are pregnant.
- The fact that drugs classified as categories C, D and Z are contraindicated for women who are pregnant.
Correct Response: A
Drugs classified as categories C, D and X are contraindicated for women who are pregnant because of the risks associated with these categories in terms of the developing fetus when these medications cross the placental barrier.
- The nurse must be knowledgeable about the fact that this client has A and B agglutinins and lacks the Rh factor
- The nurse must be knowledgeable about the fact that this client has B and O agglutinins and lacks the Rh factor
- The nurse must be knowledgeable about the fact that this client has B agglutinins and lacks the Rh factor
- The nurse must be knowledgeable about the fact that this client has A agglutinins and lacks the Rh factor
Correct Response: D
The nurse must be knowledgeable about the fact that this client has A agglutinins and they lack the Rh factor.
Type A blood has B agglutinins; type B blood has A agglutinins, type AB blood has no antibodies, or agglutinins, and type O blood has both A and B agglutinins.
People also have a rhesus, or Rh, factor antigen or the lack of it. Clients with an Rh positive blood, which is the vast majority of people, have Rh positive blood and people without the Rh factor antigen have Rh negative blood.
- Hemolysis: Typing and cross matching the blood and checking for ABO compatibility prior to administration
- Hemolysis: Insuring that the client does not have a prior history of hemolysis in the past
- Febrile reactions: Insuring that the client does not have a prior history of hemolysis in the past
- Febrile reactions: Typing and cross matching the blood and checking for ABO compatibility prior to administration
Correct Response: A
Hemolysis can be prevented by typing and cross matching the blood and checking for ABO compatibility prior to administration. This incompatibility can occur as the result of a laboratory error in terms of typing and cross matching and a practitioner error in terms of checking the blood and matching it to the client’s blood type.
Febrile reactions are the most commonly occurring reaction to blood and blood products administration. Although a febrile reaction can occur with all blood transfusions, it is most frequently associated with packed red blood cells and this reaction is not accompanied with hemolysis nor is it associated with its occurrence.
- You must insure that the client has a patent intravenous catheter that is at least 20 gauge.
- You will need the help of another nurse prior to the administration of these packed red blood cells.
- The unit of packed red blood cells should start no more than 1 hour after it is picked up.
- You must remain with and monitor the client for at least 30 minutes after the transfusion begins.
Correct Response: B
You will need the help of another nurse prior to the administration of these packed red blood cells. Two nurses must check the blood, the doctor’s order, the ABO compatibility and the client’s identity using at least two unique identifiers prior to the administration of this blood.
You must insure that the client has a patent intravenous catheter that is at least 18 gauge and not 20 gauge; you will be using normal saline and a Y infusion set for the administration of the blood because Ringer’s lactate and other intravenous solutions are not compatible with blood; blood should not remain in the client care area for more than 30 minutes so it is important that the nurse is prepared to begin the transfusion shortly after the blood is delivered to the patient care area; and, lastly, the nurse should remain with and monitor the client for at least 15 minutes after the transfusion begins at a slow rate since most serious blood reactions and complications occur shortly after the transfusion begins.
- A percutaneous, non tunneled subclavian catheter
- A peripheral intravenous catheter that is 20 gauge
- A multi lumen implanted tunneled and cuffed central venous catheter
- A peripherally inserted central venous catheter
Correct Response: C
You would most likely anticipate that this client will be given a multi lumen implanted tunneled and cuffed central venous catheter because this multi trauma client is in need of multiple intravenous therapies such as blood, medications and total parenteral nutrition over an extended period of time.
A percutaneous, non tunneled subclavian catheter would not be the device of preference because percutaneous, non tunneled subclavian catheters are used when short term treatments are anticipated; a peripheral intravenous catheter that is at least 18 gauge is necessary for the administration of blood; and a peripherally inserted central venous catheter would also not be the venous access device of choice for this seriously ill client who will require long term treatments and care.
- 1.5 tablets
- 1.25 tablets
- 1.33 tablets
- 1 tablet
Correct Response: C
You have to determine how many tablets the patient will take if the doctor has ordered 200 mg a day and the tablets are manufactured as 150 mg per tablet.
The mathematical rule for this type of calculation is:
Have = Desired
Quantity X
This problem is calculated as shown below.
200 mg: X tablets = 150 mg: 1 tablet
Or as
200 mg = 150 mg
X tablets 1 tab
You will criss cross multiply the known numbers and then divide this product by the remaining number to solve for X, as below.
200 x 1 = 150 X
200/150 = 1.33 tabs rounded off to 1 1/3 tabs
- 0.8 mL
- 0.9 mL
- 0.75 mL
- 0.125 mL
Correct Response: A
You have to determine how many mLs the patient will take if the doctor has ordered 10 mg twice a day and there are 12 mg in each mL.
The mathematical rule for this type of calculation is:
Have = Desired
Quantity X
This problem is calculated as shown below.
10 mg: X mL = 12 mg: 1 mL
Or as
10 mg = 12 mg
X mL 1 mL
You will criss cross multiply the known numbers and then divide this product by the remaining number to solve for X, as below.
10 x 1 = 10 X
10/12 = 0.833 mL rounded off to 0.8 mL
- 1.4 mL
- 1.5 mL
- 1.475 mL
- 1.425 mL
- 1.375 mL
Correct Response: A
You have to determine how many mLs the patient will take if the doctor has ordered 6,500 units of heparin subcutaneously and there are 4,500 units in one mL.
The mathematical rule for this type of calculation is:
Have = Desired
Quantity X
This problem is calculated as shown below.
6,500 units: X mL = 4,500 units: 1 mL
Or as
6,500 units = 4,500 units
X mL 1 mL
You will criss cross multiply the known numbers and then divide this product by the remaining number to solve for X, as below.
6,500 x 1 = 6,500
6,500/4,500 = 1.44 mL which is rounded off to 1.4 mL
- 45 mg
- 60 mg
- 52 mg
- 55 mg
Correct Response: D
To calculate the number of mg that this pediatric client will receive in each dose, you will have to calculate the client’s weight in kg and then determine the total mg for the day after which you will divide the daily dosage by 2 because the order is for two equally divided doses each day.
The steps for this calculation are shown below:
This is how to determine the client’s weight in terms of kg:
48 pounds: x kg = 2.2 pounds: 1 kg
Or as
48 pounds = 2.2 pounds
x kg 1 kg
You will criss cross multiply the known numbers and then divide this product by the remaining number to solve for X, as below.
48 x 1 = 48
48/2.2 = 21.81 or 21.81 kg
This is how to determine the client’s total daily dosage when the doctor has ordered has ordered 5 mg/kg/day:
21.81 kg x 5 = 109.05 mg per day
This is how to determine the client’s dose for each of the two divided doses:
109.05/2 = 54.53 mg which is rounded off to 55 mg for each of two divided doses.
- 31 gtts
- 42 gtts
- 48 gtts
- 51 gtts
Correct Response: B
The first step of this calculation is to calculate the number of mLs, or cc s, per hour and then determine the number of drops per minute. This calculation is done as follows:
1000 ml = 125 mL per hour
8 hrs
The next step is done using this rule that reflects the fact that there are 60 minutes per hour in order to determine the number of mLs per minute .
1 hour = The ordered mL per hour 125 mLs
X min 60 min
1 hour = 125 mL
X min 60 min
60 x 1 = 60
88/60 = 2.08 mL per minute
Finally, the number of drops per minute is calculated by using the intravenous infusion set’s drop factor by using this rule.
Volume per minute x Drop factor
2.08 x 20 = 41.6 gtts per minute which is rounded off to 42 gtts per minute
- 1.9 mL
- 2.0 mL
- 2.5 mL
- 2.1 mL
Correct Response: D
With this type of calculation, the amount of normal saline that will be added to a powder in a vial to reconstitute the medication is important, instead, it is the amount of medication that results after the addition of the normal saline. For example, this reconstituted medication yields it is the yield of 12 mg in an mL that is relevant. It is this that will be used in the calculation.
This calculation is done as shown below:
12 mg = 25 mg
1 mL X mL
25 x 1 = 25
25/12 = 2.08 mL which is 2.1 mL rounded off
- 0 mL
- 5 mL
- 10 mL
- 7.5 mL
Correct Response: A
When the doctor has ordered 1200 mLs of intravenous fluid every 8 hours, you would calculate the number of mLs per hour, as below.
1200/8 = 150 mLs per hour
From 8 am to 12 noon there are 4 hours so:
150 mLs x 4 = 600 mLs
Because you had 600 mLs at 8 am, you should be prepared to hand another intravenous bag because this 600 mLs should all be infused at 12 noon.
- Question the order because Benadryl is an antihistamine and not a sleeping medication.
- Refuse to give the Benadryl because this medication is a stimulant.
- Question the order because Benadryl is contraindicated when the client has a sleep inducement disorder.
- Give the Benadryl because sleep inducement is an accepted off label use of this medication.
Correct Response: D
You would administer this Benadryl because sleep inducement is an accepted off label use of this medication. When a medication is used for any other than these established and approved uses, this usage is referred to as an “off label use”.
- The “right” verification
- The “right” to refuse
- The “right” documentation
- The “right” client education
Correct Response: A
The “right verification” is not one of the “Ten Rights of Medication Administration”. The verification of the doctor’s order for a medication is to confirm the right paint, medication, dose, route and time or frequency, it, in itself, is not one of the “10 Rights”.
The “Ten Rights of Medication Administration” are the right, or correct:
- Medication
- Dose
- Time or frequency
- Patient
- Route
- Client education
- Documentation
- Right to refuse
- Assessment and
- Evaluation
- Gluteus maximus muscle.
- Vastus lateralis muscle.
- Deltoid muscle.
- The sternocledomastoid muscle.
Correct Response: B
The administration of an intramuscular injection to a neonate should be given in the vastus lateralis, rectus femoris and ventrogluteal muscle sites and not the deltoid or the gluteus maximus muscles because these muscles have not yet developed.
The sternocledomastoid muscle is not an intramuscular injection site.
- A subcutaneous injection site
- The PQRST technique
- The Z track technique
- The sublingual site
Correct Response: C
You would expect to use to use the Z track technique to administer ferrous sulfate.
Ferrous sulfate IM is given using the Z Track technique to avoid the leakage and dark staining of the injection site with this medication.
Ferrous sulfate is not administered with a subcutaneous injection or using the sublingual route. Lastly, the PQRST method is used to assess pain and not used as a guideline for medication administration.
- 1,5,4,2,3,6
- 4,3,2,6,1,5
- 4,2,5,3,1,6
- 1,5,3,6,4,2
Correct Response: A
The steps for mixing NPH, the long acting insulin, with regular insulin, the short acting insulin in the correct sequential order are:
- Prep the top of the longer acting insulin vial with an alcohol swab.
- Inject air that is equal to the ordered dosage of the longer acting insulin using the insulin syringe. Do NOT withdraw the longer acting insulin yet.
- Prep the top of the shorter acting insulin with an alcohol swab
- Inject air that is equal to the ordered dosage of the shorter acting insulin using the same insulin syringe.
- Withdraw the ordered dosage of the shorter acting insulin using the same insulin syringe.
- And, then lastly, withdraw the ordered dosage of the longer acting insulin using the same insulin syringe.
- Allow the nurse to administer the injection.
- Ask the nurse to use the vastus lateralis muscle instead.
- Ask the nurse to verify the doctor’s order again.
- Stop the nurse from administering the injection.
Correct Response: D
You would stop the nurse from administering the injection when you observe that the nurse has palpated the gluteus maximum muscle to determine the correct site. Intramuscular injection sites are determined by using boney landmarks and not by palpating the muscle.
You would not allow the nurse to administer the injection and you would not ask the nurse to use the vastus lateralis muscle instead because nothing indicates the need to do so. Lastly, you would verify the doctor’s order prior to entering the room and preparing to administer the injection and not during the time that the intramuscular site is being identified.
- You have failed to have another nurse witness the 0.8 mLs and the 0.2 mLs of waste.
- You have failed to have another nurse witness the 0.8 mLs of waste.
- You have failed to have another nurse witness the 0.2 mLs of waste.
- You have failed ask another nurse to verify the calculation of the dosage.
Correct Response: A
You have failed to have another nurse witness the 0.8 mLs and the 0.2 mLs.
All controlled substances are documented on the narcotics record as soon as they are removed, and all controlled substances that are wasted for any reason, either in its entirety or only partially, must be witnessed or documented by the wasting nurse and another nurse. Both nurses document this wasting.
It should not be necessary for you to ask another nurse to verify this calculation; the nurse is accountable and responsible for accurate dosage calculations.
- 3,2,1,4,6
- 2,1,4,5,6
- 1,2,3,5,4
- 4,1,3,2,6
Correct Response: B
The procedure for this medication reconciliation process is:
2. Compile a list of current medications and other preparations
1. Compile a list of newly prescribed medications
4. Compare the two lists and make note of any discrepancies and inconsistencies
5. Employ critical thinking and professional judgments during the comparisons of the two lists
6. Communicate and document the new list of medications to the appropriate healthcare providers
- The client with heart failure who is receiving Ringer’s lactate
- The client with cancer who is receiving bendamustine
- The client who is receiving potassium supplementation intravenously
- The client who is receiving total parenteral nutrition
Correct Response: B
The client with cancer who is receiving bendamustine is at greatest risk for extravasation. Extravasation occurs when vesicant and other vein irritating drugs infiltrate into the tissue. In severe cases, extravasation can lead to necrosis and the loss of an affected limb. Bendamustine is a vesicant chemotherapy drug.
Extravasation is not associated with the intravenous administration of Ringers lactate or potassium supplementation intravenously because this solution and medication are not vesicants. These intravenous preparations can lead to infiltration but not extravasation. Lastly, the client who is receiving total parenteral nutrition is at risk for other complications such as infection, but not extravasation.
- Infection: Lowering the limb to promote circulation
- Infiltration: The application of cold to the site
- Extravasation: The aspiration of contents including blood from the IV cannula
- Hematoma: The administration of dexrazonxane
Correct Response: C
In addition to other interventions, intravenous fluid contents including blood are aspirated from the IV cannula.
Other interventions include immediate cessation of the infusion, elevating the limb, applying warm compresses initially to rid the area of any remaining drug that is in the tissues which is then followed by cool compresses to reduce any swelling, and the administration of an ordered substance specific medication such as dexrazoxane.
One of the interventions for infection include the elevation, not lowering, of the affected limb; infiltration is treated with the application of warm, not cold, compresses and one of the interventions for hematoma is the application of pressure and heat and not the administration of dexrazonxane.
- Assess motor functioning.
- Assess sensory functioning.
- Evaluate responses to a tactile stimulation.
- Evaluate responses to a pain analgesic.
Correct Response: D
The CRIES scale is used to evaluate the neonate’s response to a pain analgesic; this pain scale is also used to assess pain among neonates.
Observational behavioral pain assessment scales for the pediatric population are used among children less than three years of age. Some of these standardized pediatric pain scales, in addition to the CRIES scale, include the FACES Pain Scale, the Toddler Preschooler Postoperative Pain Scale (TPPPS), the Neonatal Infant Pain Scale (NIPS), the Children's Hospital of Eastern Ontario Pain Scale (CHEOPS), the Faces Legs Activity Cry Consolability Pain Scale (FLACC), the Visual Analog Scale (VASobs) the Observation Scale of Behavioral Distress (OSBD), the COMFORT Pain Scale and the Pre-Verbal Early Verbal Pediatric Pain Scale (PEPPS) that is used with toddlers.
- Opioid Agonist: Dilaudid: Constipation
- Opioid Agonist: Naloxone: Constipation
- Opioid Antagonist: Dilaudid: Anaphylaxis
- Opioid Antagonist: OxyContin: Anaphylaxis
Correct Response: A
Dilaudid is an opioid agonist that can cause constipation.
Other opioid agonists are codeine, OxyContin, Darvon, Dilaudid, Demerol and Percocet. The side effects and adverse reactions to this classification of drugs include constipation, sedation, nausea, dizziness, pruritus, and sedation, respiratory depression and arrest, hepatic damage, an anaphylactic reaction, circulatory collapse and cardiac arrest.
Opioid antagonists also referred to as opioid receptor antagonists, such as naloxone and naltrexone, can have side effects such as hepatic damage, joint pain, insomnia, vomiting, anxiety, headaches and nervousness.
- Your client may be experiencing a fluid overload.
- Your client may be experiencing an embolus.
- Your client may be hyperglycemic.
- Your client may have an inadvertent pneumothorax.
Correct Response: B
The client may be experiencing an embolus, which is a complication of total parenteral nutrition. Some of the signs and symptoms of an embolus are chest pain, dyspnea, shortness of breath, coughing, and respiratory distress.
Emboli, secondary to total parenteral nutrition occur when air is permitted to enter this closed system during tubing changes and when a new bottle or bag of hyperalimentation is hung. This complication can be prevented by instructing the client to perform the Valsalva maneuver and the nurse’s rapid changing of tubings and solutions when the closed system is opened to the air.
An inadvertent pneumothorax can occur and become symptomatic during the insertion of the TPN catheter and not four days later.
Other side effects of TPN and their signs and symptoms are listed below.
- Infection: The classical signs of infection including a fever, malaise, swelling and redness at the insertion site, diaphoresis, chilling and pain in the area of the TPN catheter insertion site.
- Fluid overload: Hypertension, edema, adventitious breath sounds like crackles and rales, shortness of breath, and bulging neck veins.
- Hyperglycemia: High blood glucose levels, thirst, excessive urinary output, headache, nausea and fatigue.
- Hypoglycemia: Low blood glucose levels, shakiness, clammy and cool skin, blurry vision, diaphoresis and unconsciousness and seizures.
- Clients are at high risk for infection when they are getting TPN because they are immunocompromised.
- Clients are at high risk for hyperglycemia when they are getting TPN because they are diabetic.
- The client should perform the Valsalva maneuver when the nurse changes the TPN tubing.
- The client should perform the Valsalva maneuver when the nurse changes the TPN dressing.
Correct Response: C
The client should perform the Valsalva maneuver when the nurse changes the TPN tubing to prevent an embolus which can occur when the tubing is opened to the air while it is being changed.
A mask, not the Valsalva maneuver, is indicated for TPN dressing changes.
Lastly, clients are at risk for infection secondary to TPN because these solutions are high in dextrose and because TPN is an invasive sterile procedure; and clients are at high risk for hyperglycemia when they are getting TPN because these solutions are high in dextrose and not because the client is already a diabetic client.
Physiological Integrity: Reduction of Risk Potential Practice Questions
- Respiratory rate: 32 breaths per minute
- Pulse: 110 beats per minute
- Blood pressure: 55/82
- “The respiratory rate is a little too fast but the other vital signs are normal.”
- “The pulse rate is a little too fast but the other vital signs are normal.”
- “The blood pressure is a little low but the other vital signs are normal.”
- “All of these vital signs are normal for a child that is 2 years of age.”
Correct Response: D
All of these vital signs are normal for the toddler who is 2 years old. The normal vital signs for the toddler are:
- Respiratory rate: From 20 to 40 per minute
- Pulse rate: From 90 to 140 beats per minute
- Blood pressure: Diastolic from 50 to 80 mm Hg and systolic from 80 to 112 mm Hg
- Respiratory rate: 32 breaths per minute
- Pulse: 100 beats per minute
- Blood pressure: 85/55
- “The respiratory rate is a little too fast but the other vital signs are normal.”
- “The pulse rate is a little too fast but the other vital signs are normal.”
- “The blood pressure is a little low but the other vital signs are normal.”
- “All of these vital signs are normal for a child that is 2 years of age.”
Correct Response: A
The respiratory rate is a little too fast for this 5 year old preschool client. The normal respiratory rate for this client should be from 22 to 30 per minute.
The normal pulse rate and blood pressure for the preschool child are from 80 to 110 beats per minute and a diastolic from 50 to 78 mm Hg and a systolic from 82 to 110 mm Hg.
- Pulmonary Artery Systolic Pressure: 22 mm Hg
- Pulmonary Artery Wedge Pressure: 22 mm Hg
- Pulmonary Artery Diastolic Pressure: 10 mm Hg
- Central Venous Pressure: 5 mm Hg
Correct Response: B
You would report the pulmonary artery wedge pressure of 22 mm Hg because the normal pulmonary artery wedge pressure is from 4 to 12 mm Hg.
The other normal hemodynamic values are:
- Pulmonary Artery Systolic Pressure: 15 to 26 mm Hg
- Pulmonary Artery Diastolic Pressure: 5 to 15 mm Hg
- Central Venous Pressure: 1 to 8 mm Hg
- The need to cleanse the perineal area with circular wipes.
- The need to cleanse the perineal area from the “dirtiest” to the “cleanest”.
- The need to use a new antiseptic wipe for each wipe from the inner to the outer labia.
- The need to use a new antiseptic wipe for each wipe from the outer to the inner labia.
Correct Response: C
You would instruct your female client to use a new antiseptic wipe for each wipe from the inner to the outer labia.
A principle of asepsis is the cleansing of areas from the cleanest to the dirtiest and NOT the reverse; therefore, the inner labia are cleansed before the outer labia. The female perineal area is prepped with straight strokes and wipes; and the male wipes with a circular pattern around the urinary meatus.
- Turn the finger down so the blood will drop with gravity.
- Wipe off the first drop of blood using sterile gauze.
- Prick the side of the finger using the lancet.
- Prick the pad of the finger using the lancet.
Correct Response: D
Pricking the pad of the finger using the lancet is NOT a step in the procedure for obtaining a blood glucose sample for testing. Instead, the side of the finger is pricked with the lancet.
The procedure for checking the client’s blood glucose levels in correct sequential order is as follows:
- Verify and confirm that the code strip corresponds to the meter code.
- Disinfect the client’s finger with an alcohol swab.
- Prick the side of the finger using the lancet.
- Turn the finger down so the blood will drop with gravity.
- Wipe off the first drop of blood using sterile gauze.
- Collect the next drop on the test strip.
- Hold the gauze on the client’s finger after the specimen has been obtained.
- Read the client’s blood glucose level on the monitor.
- PaO2: 65 mm Hg
- PaCO2: 40 mm Hg
- Arterial blood pH: 7.39
- SaO2: 96%
Correct Response: A
You would report the client’s PaO2 of 65 mm Hg because it is not within normal parameters and it is also a significant change for the client. The normal partial pressure of oxygen (PaO2) is from 75 to 100 mm Hg.
The other blood gases, above, are within normal limits, as follows:
- Partial pressure of carbon dioxide (PaCO2): 38 - 42 mmHg
- Arterial blood pH: 7.38 - 7.42
- Oxygen saturation (SaO2): 94 - 100%
- Triglycerides: 75 mg/dL
- Total cholesterol: 6.5 mmol/L
- High-density lipoprotein (HDL): 60 mg/dL
- Low-density lipoprotein (LDL): 955 mg/dL
Correct Response: B
You would report a total cholesterol level of 6.5 mmol/L because this value exceeds the high normal for total cholesterol which is 5.5 mmol/L and the normal range is from 3 to 5.5 mmol/L.
The other lipid levels are normal as follows:
- Triglycerides: 50-150 mg/dL
- High-density lipoprotein (HDL): 40-80 mg/dL
- Low-density lipoprotein (LDL): 85-125 mg/dL
- Albumin: 40 g/L
- Amylase: 40 U/L
- Direct bilirubin: 17 µmol/L
- Total bilirubin: 17 µmol/L
Correct Response: C
You would report a direct bilirubin level of 17 µmol/L because this value exceeds the high normal for direct bilirubin which is 6 µmol/L and the normal range is from 0-6 µmol/L.
The other gastrointestinal related normal laboratory values are as follows:
- Albumin: 35-50 g/L
- Amylase: 30-125 U/L
- Total bilirubin: 2-20 µmol/L
- A 76 year old female client who has a history of alcohol abuse.
- A 76 year old female client who has a history of radon gas exposure.
- A 64 year old male client who has a history of cigarette smoking.
- A 64 year old male client who has hypotension.
Correct Response: D
A 64 year old male client who has hypotension is at greatest risk for impaired vascular perfusion.
Other risk factors associated with impaired vascular and tissue perfusion are:
- Hypervolemia
- Hypovolemia
- Low hemoglobin
- An immobilized limb
- Hypoxia
- Decreased cardiac output
- Diabetes
- Impaired oxygen transportation
- Hypoventilation
Alcohol abuse, cigarette smoking and exposures to radon place people at risk for cancer, rather than impaired perfusion.
- A 76 year old female client who has a history of alcohol abuse.
- A 76 year old female client who has a history of diabetes.
- A 64 year old male client who has a history of impaired oxygen transport.
- A 64 year old male client who has hypotension.
Correct Response: A
The client who is at greatest risk for the development of cancer is the 76 year old female client who has a history of alcohol abuse. Data indicates that alcohol abuse can lead to cancer of the liver and other cancers.
Diabetes, a history of impaired oxygen transport and hypotension are risk factors associated with poor tissue perfusion, and not cancer.
- The level of pain among school age children.
- The risk for the impairment of skin integrity.
- Levels of muscular strength.
- Levels of mobility.
Correct Response: B
The Norton Scale measures the client’s risk for the impairment of skin integrity. The Norton Scale and the Braden Scale are standardized tools to screen clients for their risk of skin breakdown, pressure ulcers and an impairment of skin integrity.
Pain levels among school age children are measured with other standardized pain tools for pediatric clients; and levels of muscular strength and mobility are measured also with other standardized tests and not the Norton Scale.
- Pressure
- Shearing
- Impaired tissue perfusion
- Friction
Correct Response: C
Impaired tissue perfusion is an intrinsic, or internal, risk factor that places the client at risk for pressure ulcers.
Pressure, shearing and friction are extrinsic, or external, risk factors that places the client at risk for pressure impaired tissue perfusion.
Other intrinsic risk factors associated with skin breakdown include:
- Poor nutritional status
- Immobility
- A decreased level of consciousness including that which occurs with sedating medications
- Fecal and/or urinary incontinence
- Impaired circulation
- Alterations in terms of the fluid balance
- Altered neurological sensory functioning
- Changes in terms of skin turgor
- Boney prominences
- Inflate the cuff if the cuff is deflated.
- Deflate the cuff if the cuff is inflated.
- Remove the inner cannula of the tube.
- Call the doctor about this airway obstruction.
Correct Response: B
The first thing that you should do when you insert the suction catheter and you reach a point of resistance is to deflate the cuff when it is inflated and the second thing that you should do is to remove the inner cannula and suction out the mucous plug.
You would not call the doctor because there is an airway obstruction; you should correct this problem with the measures above.
- Maintain the client with NPO status for at least 4 hours prior to this procedure.
- Teach the client about the fact that they may experience muscle flaccidity.
- Teach the client about the fact that they may have a headache after the ECT.
- Maintain the client on continuous hemodynamic monitoring after the ECT.
Correct Response: C
You would teach the client about the fact that they may have a headache after the ECT. Other components of the teaching about the aftermath of the procedure that the client should know about include the fact that the client may have muscle soreness, not muscle flaccidity, confusion, amnesia and hypertension.
The client should be maintained as NPO for at least 6 hours before ECT; and it is not necessary to maintain the client on continuous hemodynamic monitoring after the ECT, however, the client’s vital signs should be monitored.
- Strnagulation
- Skin breakdown
- Skin pallor
- Numbness
Correct Response: D
The neurological complication can occur when a vest restraint is too tight around the client’s body is numbness and tingling that, unless corrected, can lead to neurological damage.
Strangulation, skin breakdown and skin pallor can also occur when a restraint is too tight, however, these restraint complications are respiratory, integumentary system and circulatory system complications rather than neurological complications.
- The appearance of petechiae
- Aplastic anemia
- The appearance of thrombophlebitis
- Elevated platelets
Correct Response: A
The appearance of petechiae is a sign of thrombocytopenia which is a low platelet count. Other signs and symptoms include purpura, easy bruising, epistaxis, and spontaneous hemorrhage and bleeding.
Thrombocytopenia can occur as the result of several disorders and therapeutic treatments and interventions including aplastic anemia, HIV infection, a genetic disorder, cancer, particularly cancer that affects the bones, some viral pathogens like those that cause mononucleosis, as well as from therapeutic radiation therapy, chemotherapy and some medications such as Depakote.
- Infection
- Pneumothorax
- Aspiration
- Dyspnea
Correct Response: B
The complication that you should be aware of during the immediate post-operative period of time after a thoracentesis is a pneumothorax.
The signs and symptoms of pneumothorax and hemothorax include dyspnea, chest pain, shortness of breath and pain. The treatment of a pneumothorax includes the correction of the underlying cause whenever possible and the placement of a chest tube to remove the blood and/or air in the pleural space which will re-expand the affected lung and recreate the negative pressure of the pleural space.
Infection would not be evident during the immediate post-operative period; and, aspiration is not a complication of a thoracentesis.
- The client’s posterior tibia pulse is Grade B
- The client’s posterior tibia pulse is Grade C
- The client’s posterior tibia pulse is 1
- The client’s posterior tibia pulse is 2
Correct Response: C
You would document this finding as “The client’s posterior tibia pulse is 1”.
The strength, volume and fullness of the peripheral pulses are categorized and documented as follows:
- 0: Absent pulses
- 1: Weak pulse
- 2: Normal pulse
- 3: Increased volume
- 4: A bounding pulse
Grades and grading are not used in reference to pulses.
- The Lazarus Cognitive Appraisal Scale
- The Hamilton Rating Scale
- The McGill Scale
- The Rancho Los Amigos Scale
Correct Response: D
The tool or scale that you would use for a focused neurological assessment of your client is the Rancho Los Amigos Scale.
Levels of consciousness, which is part of a complete focused neurological assessment, can be determined and measured by using the standardized Glasgow Coma Scale for adults and children or the Rancho Los Amigos Scale. The Rancho Los Amigos Scale determines the patient’s level of awareness and functioning which can range from a 1 to an 8 when a 1 is the complete lack of all responsiveness to all stimulation and an 8 is when a patient is fully alert, oriented, appropriate and purposeful.
The McGill Pain Assessment is used to assess pain levels; the Lazarus Cognitive Appraisal Scale is used to assess levels of stress and coping; and the Hamilton Rating Scale is used to measure and assess depression.
- A lack of zinc
- A lack of vitamin E
- High iron levels
- High phosphorous levels
Correct Response: A
A lack of zinc, copper, iron and vitamins C and A are risks associated with impaired and delayed wound healing.
Other risk factors that impede wound healing are:
- Advancing age
- Nutritional status
- Some poor lifestyle choices
- Some medications
- Some diseases and disorders
- “The client is having anesthesia awareness which is not good.”
- “This often happens during stage 2 of general anesthesia.”
- "The client needs more general anesthesia.”
- “The client is having a seizure.”
Correct Response: B
You should respond to this student nurse by stating, “This often happens during stage 2 of general anesthesia.”
Stage 2 of general anesthesia, often referred to as the Excitement Stage, is characterized with uncontrollable muscular activity, irregular respirations, an irregular cardiac rhythm, and, at times, vomiting. This stage does not indicate the need for more general anesthesia.
Anesthesia awareness, which is a rare complication of general anesthesia, is the lack of amnesia during surgery when the client remembers events during surgery and, at times, they remember the pain.
Lastly, there is no evidence in this question that the client is having a seizure.
- Surgical site marking
- A time out
- Medication reconciliation
- A neutral zone for sharps
Correct Response: C
Medication reconciliation prevents medication errors and other complications associated with medications and not a way to reduce surgical risks.
Surgical marking, time outs that are done after surgical site marking is done, and a neutral zone for sharps do reduce surgical risks such as wrong site surgery, wrong patient surgeries and sharps injuries.
Physiological Integrity: Physiological Adaptation Practice Questions
- Exclude pregnant visitors from the client’s room.
- Place the client in a negative pressure room.
- Have all visitors wear protective masks and boots.
- All of the above
Correct Response: A
You would exclude all pregnant visitors from the client’s room in order to protect the pregnant woman’s developing fetus. Brachytherapy is internally placed radioactive material to treat clients who are affected with tumor and cancer of the prostate, lungs, esophagus, cervix, endometrium, rectum, breast, head and neck.
Special radiation precautions are initiated when a client is receiving brachytherapy in order to protect visitors and health care staff from the harmful effects of the radiation. Some of the other special internal radiation precautions include:
- The minimization of the duration of time that health care providers are in the client’s room to deliver care and services to the client
- The placement of the client receiving internal radiation in a private room. A negative pressure room is not indicated for this client.
- The prohibition of the client’s activities outside of their room
- The initiation of complete bed rest for the client until the treatment is discontinued
- The provision of education to the family members and other visitors that includes information about their need to limit the time of their visits to at least less than 1 hour, to stay at least 6 feet away from the client
- The need for health care staff to minimize the amount of time spent in the room, to decline to enter the room if they are pregnant, to retain all supplies and equipment including things like bed linens in the client’s room until they are deemed safe for disposal by a person who is competent to make this decision, and how and when to report concerns about the client’s treatment such as when implanted seeds inadvertently leave the client’s body.
- Fibrosis
- Alopecia
- Oral dryness
- Xerostomia
Correct Response: A
Fibrosis is an adverse effect to therapeutic radiation therapy.
Radiation fibrosis can affect bones, nerves, ligaments, muscles, blood vessels, tendons, and the heart in addition to the lungs. Fibrosis occurs as the result of abnormal fibrin and protein accumulation within normal irradiated tissue.
Alopecia, and oral dryness which is also referred to as xerostomia, are side effects and complications to radiation, but not adverse effects.
Other side effects, complications and adverse effects associated with therapeutic radiation therapy are:
- Skin damage
- Damage to the mucosa
- Dental caries and oral infections
- Fatigue
- Nausea and vomiting
- Anorexia
- Diarrhea
- Bone marrow suppression and immunosuppression
- Radiation pneumonia
- Cataracts
- Placing the client in the Trendelenburg position
- Monitoring the color of the stools
- Using a Hoyer lift for patient transfers
- Monitoring the arterial blood gases
Correct Response: B
You would monitor the color of the stools for the client who is receiving phototherapy. Phototherapy is used to treat psoriasis, but it is most commonly employed for the treatment of neonatal hyperbilirubinemia and jaundice which can occur among both full term and pre term infants.
You would also monitor and document the client’s:
- Skin for changes in color that may indicate an increase or decrease in the amount of bilirubin in the client’s blood
- Laboratory bilirubin levels to determine whether or not the client’s bilirubin levels are decreasing as the result of the phototherapy
- Volume, color and characteristics of the stool because phototherapy can lead to frequent, loose stools as well as a color change to green colored stools
- Hypokalemia: Hypermagnesemia
- Hyponatremia: Dehydration
- Hyperkalemia: Ketoacidosis
- Hypercalcemia: Hypoparathyroidism
Correct Response: C
Ketoacidosis is a risk factor for hyperkalemia.
The risk factors for the other electrolyte disorders above are listed below.
- Hypokalemia: Diarrhea, vomiting, and diaphoresis as well as some medications like diuretics and laxatives, and with other disorders and diseases such as ketoacidosis. Hypermagnesemia is not a risk factor for hypokalemia.
- Hyponatremia: Thyroid gland disorders, cirrhosis, renal failure, heart failure, pneumonia, diabetes insipidus, Addison’s disease, hypothyroidism, primary polydipsia, severe diarrhea or vomiting cancer, and cerebral disorders. Dehydration is a risk factor associated with hypernatremia, not hyponatremia.
- Hypercalcemia: Hyperparathyroidism, not hyperparathyroidism, some medications such as thiazide diuretics and lithium, some forms of cancer such as breast cancer and cancer of the lungs, with multiple myeloma, Paget’s disease, non weight bearing activity and elevated levels of calcitriol as occurs with sarcoidosis and tuberculosis.
- Hypernatremia: Hepatic failure
- Hypocalcemia: Vitamin A deficiency
- Hypermagnesemia: Cushing’s disease
- Hypomagnesemia: Crohn’s disease
Correct Response: D
Crohn’s disease is a risk factor for hypomagnesemia.
Other electrolyte disorder risk factors include:
- Hypernatremia: Dehydration, renal failure, hyperglycemia and Cushing’s disease
- Hypocalcemia: Vitamin D deficiency, Crohn’s disease, sepsis and pancreatitis
- Hypermagnesemia: Addison’s disease, renal failure, diabetic ketoacidosis and dehydration
- Phosphate: From 0.81 to 1.45 mmol/L.
- Chloride: From 60 to 110 mEq/L.
- Calcium: From 6.5 - 10.6 mg/dL.
- Potassium: From 3.7 to 7.2 mEq/L.
Correct Response: A
The normal level of phosphate is from 0.81 to 1.45 mmol/L.
The other normal levels for these electrolytes are:
- Chloride: From 97 to107 mEq/L.
- Calcium: From 8.5 - 10.6 mg/dL.
- Potassium: From 3.7 to 5.2 mEq/L.
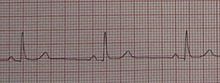
- Idioventricular Rhythm
- Bundle Branch Block
- Sinus bradycardia
- Atrial Flutter
Correct Response: C
Sinus bradycardia is a sinus rhythm that is like the normal sinus rhythm with the exception of the number of beats per minute. Sinus bradycardia has a cardiac rate less than 60 beats per minute, the atrial and the ventricular rhythms are regular, the P wave occurs prior to each and every QRS complex, the P waves are uniform in shape, the length of the PR interval is form 0.12 to 0.20 seconds, the QRS complexes are uniform and the length of these QRS complexes are from 0.06 to 0.12 seconds.

- Asystole
- Atrial flutter
- Supraventricular Tachycardia
- Premature Atrial Contractions
Correct Response: B
Atrial flutter, which is a relatively frequently occurring tachyarrhymia; this cardiac rhythm is characterized with an rapid atrial rate of 250 to 400 beats per minute, a variable ventricular rate, a regular atrial rhythm, a possibly irregular ventricular rhythm, the P waves are not normal, the flutter wave has a saw tooth look (f waves), the PR interval is not measurable, QRS complexes are uniform and the length of these QRS complexes are from 0.06 to 0.12 seconds.
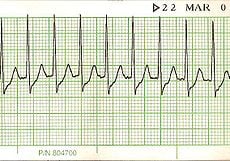
- Torsades de Pointes
- Accelerated Idioventricular Arrhythmia
- First Degree Atrioventricular Heart Block
- Supraventricular tachycardia
Correct Response: D
Supraventricular tachycardia, simply defined is all tachyarrhythmias with a heart rate of more than 150 beats per minute.
The atrial and ventricular cardiac rates are from 150 to 250 beats per minute, the cardiac rhythm is regular, the p wave may not be visible because it is behind the QRS complex, the PR interval is not discernable, the QRS complexes look alike, and the length of the QRS complexes ranges from 0.06 to 0.12 seconds.
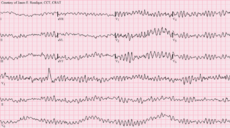
- Third Degree Heart Block
- Second-Degree Atrioventricular Block, Type II
- Ventricular fibrillation
- Premature Atrial Contractions
Correct Response: C
The two types of ventricular fibrillation that can be seen on an ECG strip are fine ventricular fibrillation and coarse ventricular fibrillation; ventricular fibrillation occurs when there are multiple electrical impulses from several ventricular site. This results in erratic and uncoordinated ventricular and/or atrial contractions.
- 100 mLs
- 250 mLs
- 400 mLs
- 500 mLs
Correct Response: B
You would instill 250 mLs of irrigating solution after each suctioning of the nasogastric tube. The typical amount of irrigating solution is from 20 mLs to 300 mLs.
- The compression of the renal medulla.
- Syncope and dizziness of unknown origin.
- Pressure on the vena cava which is a major vein in the body.
- Pressure on the vena cava which is the largest artery in the body.
Correct Response: C
You should explain that superior vena cava syndrome is pressure on the vena cava which is a major vein, not an artery, in the body that carries blood from the systemic circulation to the right atrium of the heart. This pressure on the superior vena cava prevents the normal return of the body’s circulating blood to the heart.
The signs and symptoms of superior vena cava syndrome include tachypnea, dyspnea, venous stasis, a loss of consciousness, edema, seizures, respiratory and/or cardiac arrest and not syncope of unknown origin. This is a life threatening medical emergency.
- Hypovolemic shock
- Septic shock
- A dissected thoracic aortic aneurysm
Correct Response: C
You would most likely suspect that this client is affected with a dissected thoracic aneurysm. Thoracic aorta rupture and dissections can present with symptoms that can include shortness of breath, dysphagia, dyspnea, coughing, and pain in the chest, arms, jaw, neck, and/or back.
The signs and symptoms of hypovolemic shock vary according to the stage of the shock; some of the signs and symptoms include hypotension, tachycardia, a lack of tissue perfusion, hyperventilation, decreased cardiac output, decreased urinary output, oliguria, anuria, metabolic acidosis, increased blood viscosity, and multisystem failure.
The signs and symptoms of septic shock include the classical signs of infection in addition to hypotension, confusion, metabolic acidosis, respiratory alkalosis, abnormal breath sounds like crackles and rales, a widened pulse pressure, and decreased cardiac output.
- Part of the intestine slides into another part of the intestine.
- The appendix ruptures.
- An ileostomy stoma retracts below the abdominal surface.
- Lungs are infiltrated.
Correct Response: A
Intussusception occurs when a part of the intestine slides into another part of the intestine. This medical emergency can lead to poor perfusion to the intestine.
The signs and symptoms of intussusception include knee to chest posturing, abdominal pain, bloody stool, fever, constipation, vomiting and diarrhea.
A ruptured appendix occurs when an infected appendix ruptures; a stoma retraction occurs when an ileostomy stoma retracts below the abdominal surface; and pneumonia occurs when the lungs become infiltrated.
- The administration of a thrombolytic medication
- The administration of hyroxyurea
- Placing the client in the Trendelenburg position
- Placing the client in the lithotomy position
Correct Response: B
You would expect to administer hydroxyurea which prevents the sickling of the client’s red blood cells. You would not administer a thrombolytic medication; however, you would likely administer analgesic medications for the pain associated with the sickle cell crisis.
The lithotomy position is used for procedures involving the pelvis, including gynecological examinations; and the Trendelenburg position is used when the client is in shock and with significant hypotension.
- Perform the Valsalva maneuver
- Encourage the person to continue coughing
- Perform the Heimlich maneuver
- Begin CPR and prepare for ACLS measures
Correct Response: B
You would encourage the person to continue coughing because this person has a partial airway obstruction.
You would perform the Heimlich maneuver when the person has a complete airway obstruction. CPR and ACLS may be necessary later, but not now as based on the fact that the person only has a partial airway obstruction. Lastly, the Valsalva maneuver is done when one exerts pressure against resistance.
- Trichomoniasis
- E. coli
- Staphylococcus aureus
- Neisseria gonorrhoeae
Correct Response: D
Pelvic inflammatory disease is most often caused by the Neisseria gonorrhoeae and Chlamydia trachomatis pathogens; and it most often occurs as the result of untreated salpingitis, pelvic peritonitis, a tubo ovarian abscess and/or endometritis.
Unlike Neisseria gonorrhoeae, trichomoniasis and infections caused by E. coli and Staphylococcus aureus are not associated with the onset of pelvic inflammatory disease which can lead to infertility, increased risk for ectopic pregnancies, sepsis, septic shock and death when left untreated.
- Adaptive immunity
- Passive natural immunity
- Active natural immunity
- Active artificial immunity
Correct Response: C
The type of immunity occurs when a person has an infectious, communicable disease like the measles is active natural immunity.
Active immunity occurs as the result of our bodily response to the presence of an antigen, with the development of antibodies. Active immunity can be both natural and artificial. Natural active immunity occurs when the body produces antibodies after the client is infected with a pathogen; and artificial active immunity occurs when the body produces antibodies to an immunization vaccine such as those for pneumonia and a wide variety of childhood infectious diseases.
Adaptive immunity is the acquisition of antibodies or activated T cells in the body. Passive immunity occurs when an antibody is introduced into the body by either natural or artificial means. Passive natural immunity occurs when the fetus and neonate receive immunity as a natural process through the placenta; and passive artificial immunity occurs when the client receives an injection of immune globulin.
- The incubation stage
- The illness stage
- The prodromal stage
- The convalescence stage
Correct Response: C
The prodromal stage, or phase, of the infection process is characterized with general malaise, joint and muscular aches and pains, anorexia, and the presence of a headache. The prodromal stage begins with the onset of symptoms and this stage is characterized with the replication and reproduction of the pathogen.
The incubation stage is asymptomatic; the illness stage is the period of time that begins with continuation of the signs and symptoms and it continues until the symptoms are no longer as serious as they were before; and the convalescence stage is the period of recovery during which time the symptoms completely disappear.
- They are not as effective as regular defibrillators.
- They are replacing regular defibrillators in acute care settings.
- Only BLS certified people in the community should use them.
- They can be easily used by people with no healthcare experience.
Correct Response: D
Automated external defibrillators can be easily used by people with no healthcare experience. Automated external defibrillators are simple to use and there is no need to be able to recognize cardiac arrhythmias or interpret cardiac rhythm strips. Automated external defibrillations are intended to be used by the general public without any healthcare or nursing knowledge of experience; therefore, they are not restricted to only those BLS certified.
Although they are highly effective, they are not replacing the standard defibrillators in the acute care setting.
- Episiotomy extension related to a forceps delivery
- Respiratory depression related to NSAIDs
- Hemothorax related to a latex allergy
- All of the above
Correct Response: A
Maternal trauma, lacerations, pelvic floor damage, bleeding and an inadvertent extension of the episiotomy to the anus when a forceps delivery of a new born is done.
Respiratory depression can occur as the result of narcotic analgesics such as morphine, and not NSAIDs; pneumothorax and hemothorax can occur as the result of an inadvertent perforation during invasive procedures such as the placement of a total parenteral nutrition catheter and a thoracentesis; and the signs and symptoms of a latex allergy include tachycardia, hypotension, dyspnea, chest pain tremors, and anaphylactic shock, not respiratory depression.